

Nomogram for prediction of the international study Group of Liver Surgery (ISGLS) grade B/C Posthepatectomy liver failure in HBV-related hepatocellular carcinoma patients: an external validation and prospective application study
- PMID: 33115425
- PMCID: PMC7592579
- DOI: 10.1186/s12885-020-07480-2
Nomogram for prediction of the international study Group of Liver Surgery (ISGLS) grade B/C Posthepatectomy liver failure in HBV-related hepatocellular carcinoma patients: an external validation and prospective application study
Abstract
Background: To develop a nomogram for predicting the International Study Group of Liver Surgery (ISGLS) grade B/C posthepatectomy liver failure (PHLF) in hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) patients.
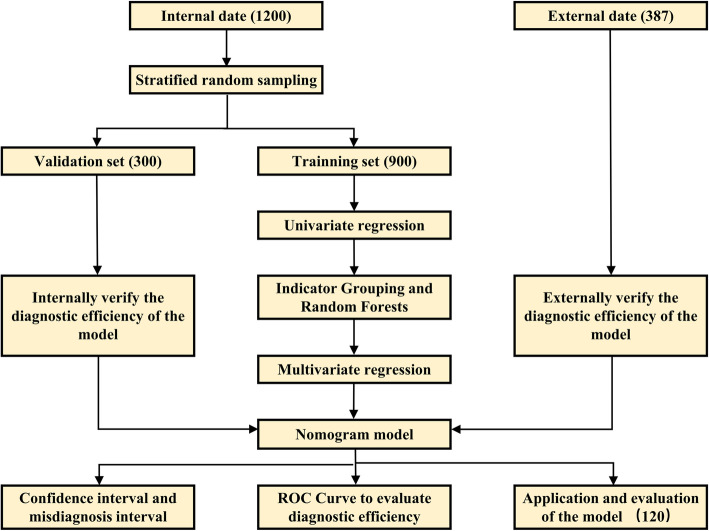
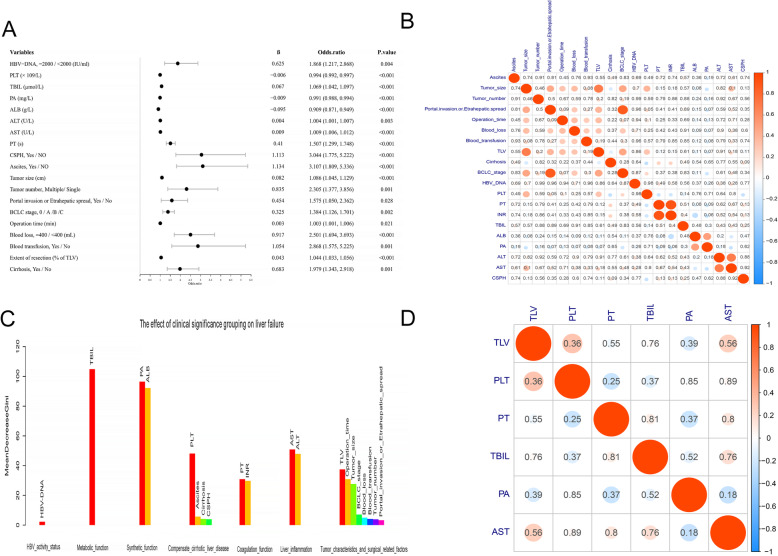
Methods: Patients initially treated with hepatectomy were included. Univariate regression analysis and stochastic forest algorithm were applied to extract the core indicators and reduce redundancy bias. The nomogram was then constructed by using multivariate logistic regression, and validated in internal and external cohorts, and a prospective clinical application.
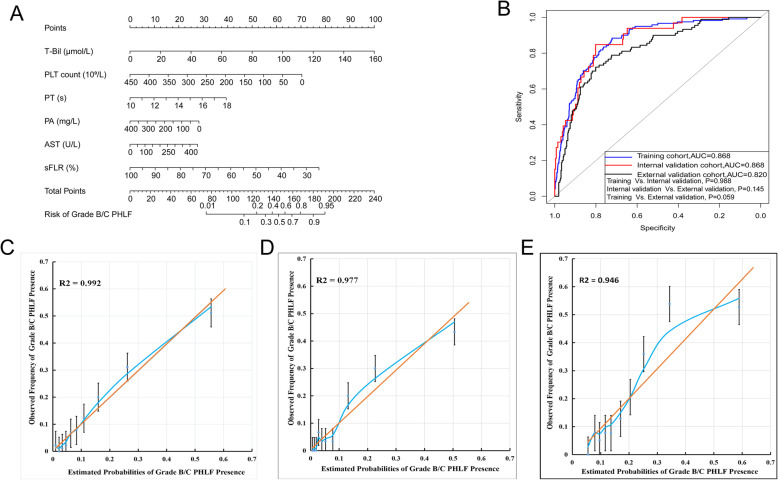
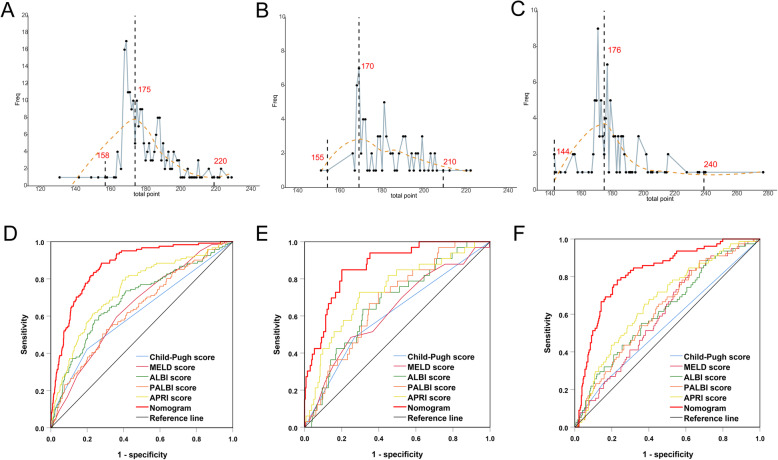
Results: There were 900, 300 and 387 participants in training, internal and external validation cohorts, with the morbidity of grade B/C PHLF were 13.5, 11.0 and 20.2%, respectively. The nomogram was generated by integrating preoperative total bilirubin, platelet count, prealbumin, aspartate aminotransferase, prothrombin time and standard future liver remnant volume, then achieved good prediction performance in training (AUC = 0.868, 95%CI = 0.836-0.900), internal validation (AUC = 0.868, 95%CI = 0.811-0.926) and external validation cohorts (AUC = 0.820, 95%CI = 0.756-0.861), with well-fitted calibration curves. Negative predictive values were significantly higher than positive predictive values in training cohort (97.6% vs. 33.0%), internal validation cohort (97.4% vs. 25.9%) and external validation cohort (94.3% vs. 41.1%), respectively. Patients who had a nomogram score < 169 or ≧169 were considered to have low or high risk of grade B/C PHLF. Prospective application of the nomogram accurately predicted grade B/C PHLF in clinical practise.
Conclusions: The nomogram has a good performance in predicting ISGLS grade B/C PHLF in HBV-related HCC patients and determining appropriate candidates for hepatectomy.
Keywords: Hepatitis B virals; Hepatocellular carcinoma; Nomogram; Posthepatectomy liver failure.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380:1450–62. - PubMed
-
- Jian-hong Z, Yang K, Wen-feng G, Bang-de X, Liang M, Xin-ping Y, et al. Hepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinoma. Ann Surg. 2014;260:329–40. - PubMed
-
- Emmanuel M, Martin H, Michael S, Chris S, James P, Dejong CHC, et al. Guidelines for perioperative Care for Liver Surgery: enhanced recovery after surgery (ERAS) society recommendations. World J Surg. 2016;40:2425–40. - PubMed
-
- Schreckenbach T, Liese J, Bechstein WO, Moench C. Posthepatectomy liver failure. Dig Surg. 2012;29:79–85. - PubMed
Publication types
MeSH terms
Grants and funding
- No:81803007/National Outstanding Youth Science Fund Project of National Natural Science Foundation of China
- No:2018GXNSFBA281030/National Outstanding Youth Science Fund Project of National Natural Science Foundation of China
- No:81730097/Natural Science Foundation of Qinghai (CN)
- No. 81521091/Science Fund for Creative Research Groups
- No:2015CB554000/Chang Jiang Scholars Programme (2013) of China Ministry of Education
LinkOut - more resources
Full Text Sources
Medical
Research Materials
