

Unusual disseminated Talaromyces marneffei infection mimicking lymphoma in a non-immunosuppressed patient in East China: a case report and review of the literature
- PMID: 33115429
- PMCID: PMC7594432
- DOI: 10.1186/s12879-020-05526-1
Unusual disseminated Talaromyces marneffei infection mimicking lymphoma in a non-immunosuppressed patient in East China: a case report and review of the literature
Abstract
Background: Talaromyces marneffei infection is an important opportunistic infection associated with acquired immune deficiency syndrome (AIDS). However, it is unusual in patients with non-AIDS and other non-immunosuppressed conditions. We report a case of delayed diagnosis of disseminated T. marneffei infection in non-AIDS, non-immunosuppressive and non-endemic conditions.
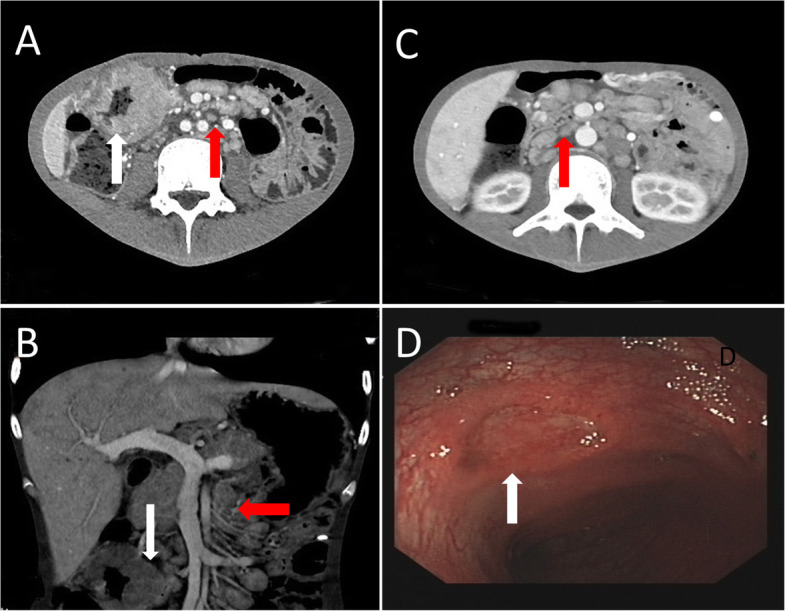
Case presentation: We describe a previously healthy 24-year-old man who complained of a 3-month history of intermittent diarrhea and a recent week of uncontrollable high fever. The HIV antibody test was negative. Enhanced abdominal computed tomography (CT) and integrated 18F-2-deoxy-2-fluoro-D-glucose position emission tomography/computed tomography (FDG PET/CT) both suspected malignant lymphoma. However, a large number of yeast-like cells were found in macrophages in cervical lymph node samples by hematoxylin and eosin stain and silver hexamine stain. Subsequent blood culture suggested T. marneffei infection. Metagenomic Next Generation Sequencing (mNGS) results suggested T. marneffei as the dominant pathogen. Unfortunately, the patient continued to develop acute liver failure and died due to adverse events associated with amphotericin B.
Conclusions: Early diagnosis in HIV-negative patients who are otherwise not immunosuppressed and endemic poses a serious challenge. T. marneffei infection is an FDG-avid nonmalignant condition that may lead to false-positive FDG PET/CT scans. Nevertheless, integrated FDG PET/CT is necessary in patients with fever of unknown origin in the early period to perform earlier biopsy for histopathology and culture in highly avid sites and to avoid delays in diagnosis and treatment.
Keywords: Delay in diagnosis; FDG PET/CT; Non-AIDS patient; Non-immunosuppressed patient; Talaromyces marneffei.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Gastrointestinal manifestations of Talaromyces marneffei infection in an HIV-infected patient rapidly verified by metagenomic next-generation sequencing: a case report.BMC Infect Dis. 2021 Apr 21;21(1):376. doi: 10.1186/s12879-021-06063-1. BMC Infect Dis. 2021. PMID: 33882850 Free PMC article.
-
Disseminated Talaromyces marneffei infection initially presenting as cutaneous and subcutaneous lesion in an HIV-Negative renal transplant recipient: a case report and literature review.BMC Infect Dis. 2024 May 6;24(1):473. doi: 10.1186/s12879-024-09351-8. BMC Infect Dis. 2024. PMID: 38711014 Free PMC article. Review.
-
Metagenomic next-generation sequencing assisted in the successful treatment of pneumonia caused by Talaromyces marneffei in an immunocompetent patient.J Infect Dev Ctries. 2024 Aug 31;18(8):1296-1300. doi: 10.3855/jidc.19061. J Infect Dev Ctries. 2024. PMID: 39288380
-
Disseminated talaromycosis in HIV-negative patients with lung cancer: a rare case report and literature review.BMC Infect Dis. 2025 Apr 24;25(1):601. doi: 10.1186/s12879-025-10985-5. BMC Infect Dis. 2025. PMID: 40275259 Free PMC article. Review.
-
Disseminated Talaromyces marneffei infection presenting as multiple intestinal perforations and diffuse hepatic granulomatous inflammation in an infant with STAT3 mutation: a case report.BMC Infect Dis. 2020 Jun 3;20(1):394. doi: 10.1186/s12879-020-05113-4. BMC Infect Dis. 2020. PMID: 32493232 Free PMC article.
Cited by
-
Nodular Sclerosing Hodgkin Lymphoma Combined with Disseminated Talaromyces marneffei Infection: A Case Report.Infect Drug Resist. 2021 Dec 24;14:5671-5678. doi: 10.2147/IDR.S340192. eCollection 2021. Infect Drug Resist. 2021. PMID: 34992393 Free PMC article.
-
Rapid Genomic Diagnosis of Fungal Infections in the Age of Next-Generation Sequencing.J Fungi (Basel). 2021 Aug 5;7(8):636. doi: 10.3390/jof7080636. J Fungi (Basel). 2021. PMID: 34436175 Free PMC article. Review.
-
Application of metagenomic next-generation sequencing in the diagnosis of infectious diseases.Front Cell Infect Microbiol. 2024 Nov 15;14:1458316. doi: 10.3389/fcimb.2024.1458316. eCollection 2024. Front Cell Infect Microbiol. 2024. PMID: 39619659 Free PMC article. Review.
-
Disseminated Combined Talaromyces marneffei and Enterococcus faecium Bloodstream Infection Presenting as Gastrointestinal Perforation in a Patient with CARD9 Gene Mutation.Infect Drug Resist. 2024 Oct 31;17:4783-4790. doi: 10.2147/IDR.S479629. eCollection 2024. Infect Drug Resist. 2024. PMID: 39498413 Free PMC article.
-
Talaromyces marneffei infection with IFNGR1 gene mutation in a patient with negative Anti-Interferon-γ autoantibodies.An Bras Dermatol. 2024 Mar-Apr;99(2):233-237. doi: 10.1016/j.abd.2023.03.006. Epub 2023 Nov 3. An Bras Dermatol. 2024. PMID: 37926601 Free PMC article.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
