

Intravenous Albumin for Mitigating Hypotension and Augmenting Ultrafiltration during Kidney Replacement Therapy
- PMID: 33115729
- PMCID: PMC8259476
- DOI: 10.2215/CJN.09670620
Intravenous Albumin for Mitigating Hypotension and Augmenting Ultrafiltration during Kidney Replacement Therapy
Abstract
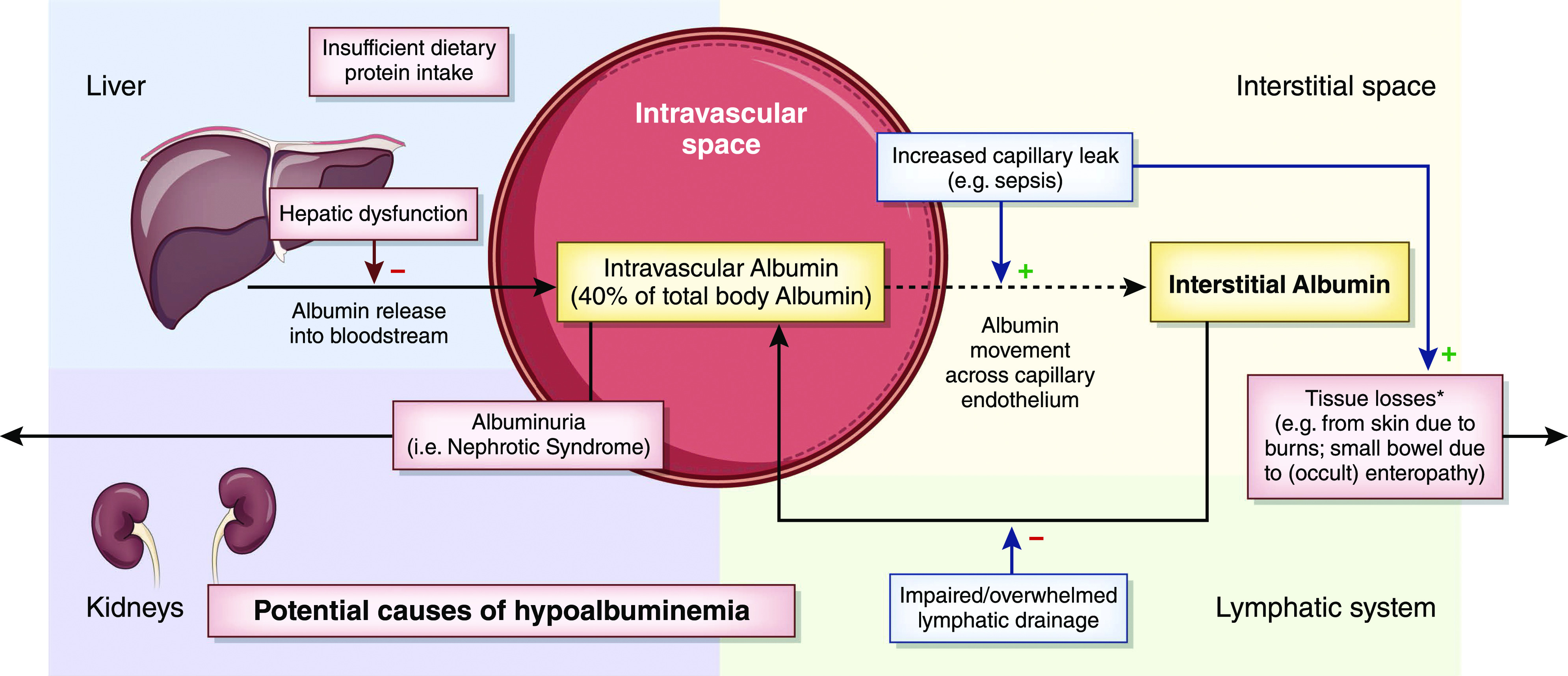
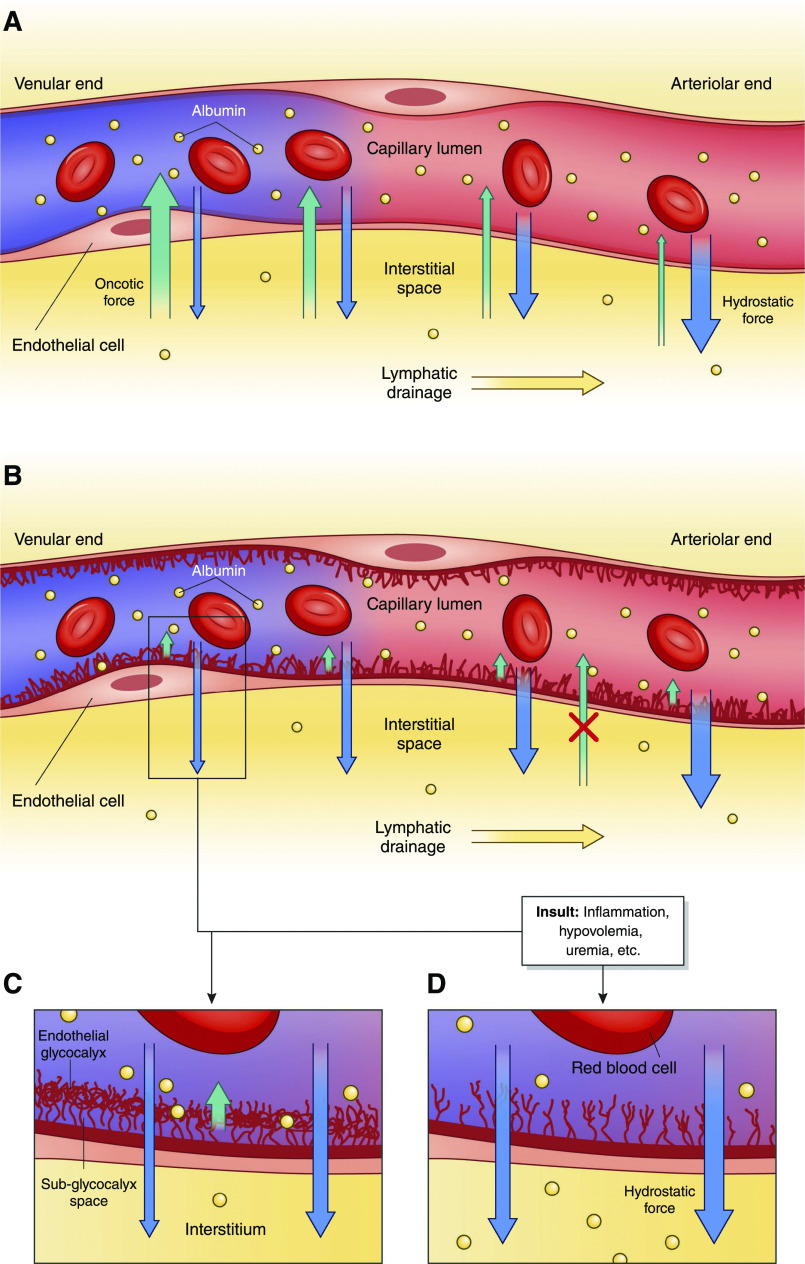
Among its many functions, owing to its oversized effect on colloid oncotic pressure, intravascular albumin helps preserve the effective circulatory volume. Hypoalbuminemia is common in hospitalized patients and is found especially frequently in patients who require KRT either for AKI or as maintenance hemodialysis. In such patients, hypoalbuminemia is strongly associated with morbidity, intradialytic hypotension, and mortality. Intravenous albumin may be administered in an effort to prevent or treat hypotension or to augment fluid removal, but this practice is controversial. Theoretically, intravenous albumin administration might prevent or treat hypotension by promoting plasma refilling in response to ultrafiltration. However, clinical trials have demonstrated that albumin administration is not nearly as effective a volume expander as might be assumed according to its oncotic properties. Although intravenous albumin is generally considered to be safe, it is also very expensive. In addition, there are potential risks to using it to prevent or treat intradialytic hypotension. Some recent studies have suggested that hyperoncotic albumin solutions may precipitate or worsen AKI in patients with sepsis or shock; however, the overall evidence supporting this effect is weak. In this review, we explore the theoretical benefits and risks of using intravenous albumin to mitigate intradialytic hypotension and/or enhance ultrafiltration and summarize the current evidence relating to this practice. This includes studies relevant to its use in patients on maintenance hemodialysis and critically ill patients with AKI who require KRT in the intensive care unit. Despite evidence of its frequent use and high costs, at present, there are minimal data that support the routine use of intravenous albumin during KRT. As such, adequately powered trials to evaluate the efficacy of intravenous albumin in this setting are clearly needed.
Keywords: acute kidney injury; albumin; chronic hemodialysis; dialysis; hemodialysis; hypotension; intradialytic hypotension; intravenous albumin; kidney replacement therapy; ultrafiltration.
Copyright © 2021 by the American Society of Nephrology.
Figures
References
-
- Carter DC, Ho JX: Structure of serum albumin. Adv Protein Chem 45: 153–203, 1994. - PubMed
-
- Doweiko JP, Nompleggi DJ: Role of albumin in human physiology and pathophysiology. JPEN J Parenter Enteral Nutr 15: 207–211, 1991. - PubMed
-
- Clarke G, Yan M: Albumin. In: Clinical Guide to Transfusion, edited by Clarke G and Chargé S, Ottawa, Canada, Canadian Blood Services, 2018, pp 1–19
-
- Cantin AM, Paquette B, Richter M, Larivée P: Albumin-mediated regulation of cellular glutathione and nuclear factor kappa B activation. Am J Respir Crit Care Med 162: 1539–1546, 2000. - PubMed
-
- Evans TW: Review article: Albumin as a drug--Biological effects of albumin unrelated to oncotic pressure. Aliment Pharmacol Ther 16[Suppl 5]: 6–11, 2002. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
