

Gastrointestinal-resident, shape-changing microdevices extend drug release in vivo
- PMID: 33115736
- PMCID: PMC7608789
- DOI: 10.1126/sciadv.abb4133
Gastrointestinal-resident, shape-changing microdevices extend drug release in vivo
Abstract
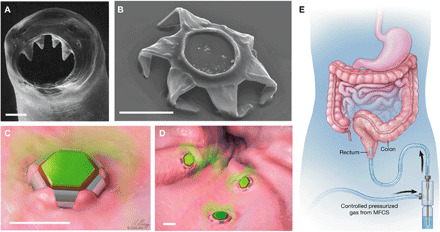
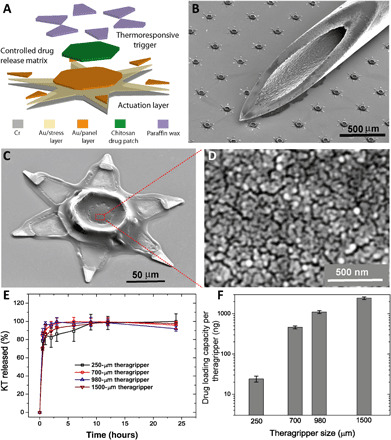
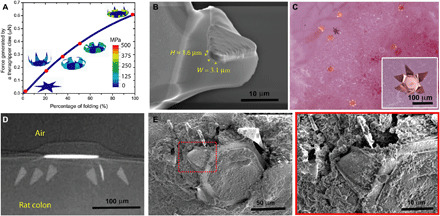
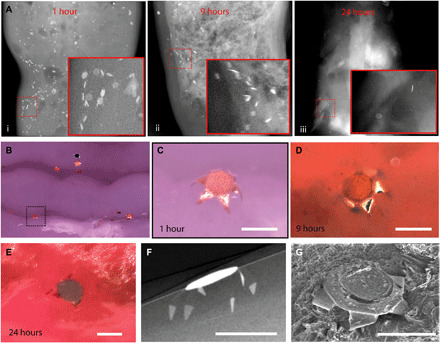
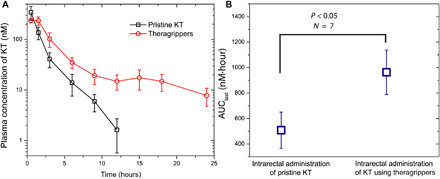
Extended-release gastrointestinal (GI) luminal delivery substantially increases the ease of administration of drugs and consequently the adherence to therapeutic regimens. However, because of clearance by intrinsic GI motility, device gastroretention and extended drug release over a prolonged duration are very challenging. Here, we report that GI parasite-inspired active mechanochemical therapeutic grippers, or theragrippers, can reside within the GI tract of live animals for 24 hours by autonomously latching onto the mucosal tissue. We also observe a notable sixfold increase in the elimination half-life using theragripper-mediated delivery of a model analgesic ketorolac tromethamine. These results provide first-in-class evidence that shape-changing and self-latching microdevices enhance the efficacy of extended drug delivery.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution License 4.0 (CC BY).
Figures
References
-
- Traverso G., Langer R., Perspective: Special delivery for the gut. Nature 519, S19 (2015). - PubMed
-
- Garg R., Gupta G. D., Progress in controlled gastroretentive delivery systems. Trop. J. Pharm. Res. 7, 1055–1066 (2008).
-
- Jannin V., Lemagnen G., Gueroult P., Larrouture D., Tuleu C., Rectal route in the 21st Century to treat children. Adv. Drug Deliv. Rev. 73, 34–49 (2014). - PubMed
-
- Lowry M., Rectal drug administration in adults: How, when, why. Nurs. Times 112, 12–14 (2016). - PubMed
-
- Healthprize, “Medication adherence: Pharma’s $637 billion opportunity”; https://healthprize.com/blog/medication-adherence-pharmas-637-billion-op....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
