

A probiotic yeast-based immunotherapy against Clostridioides difficile infection
- PMID: 33115949
- PMCID: PMC7692727
- DOI: 10.1126/scitranslmed.aax4905
A probiotic yeast-based immunotherapy against Clostridioides difficile infection
Abstract
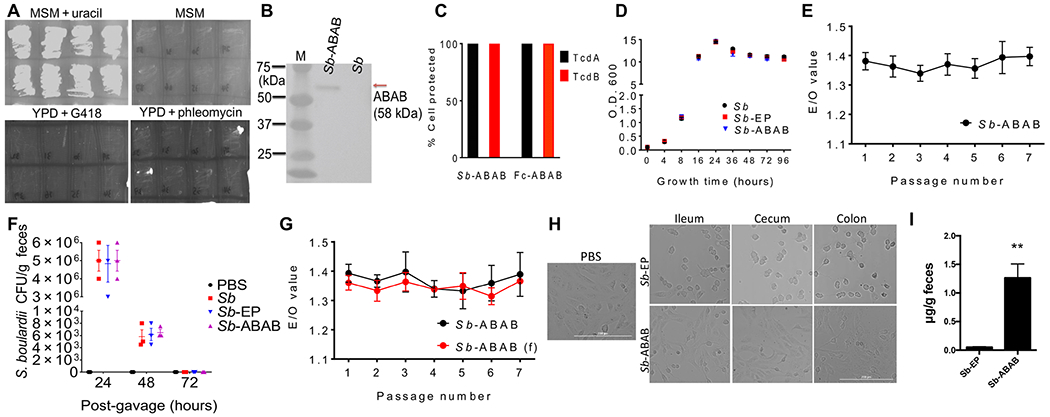
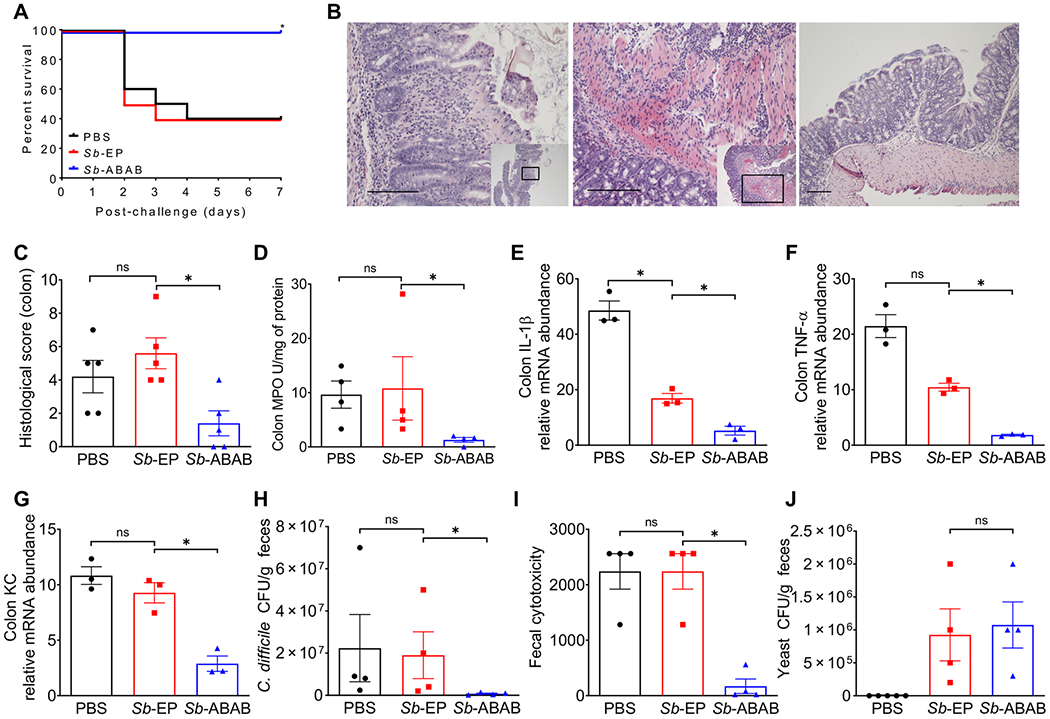
Antibiotic-resistant Clostridioides difficile is an anaerobic Gram-positive bacterium that colonizes the colon and is responsible for more than 29,000 deaths in the United States each year. Hence, C. difficile infection (CDI) poses an urgent threat to public health. Antibody-mediated neutralization of TcdA and TcdB toxins, the major virulence factors of CDI, represents an effective strategy to combat the disease without invoking antibiotic resistance. However, current antitoxin approaches are mostly based on parenteral infusion of monoclonal antibodies that are costly, narrow spectrum, and not optimized against the intestinal disease. Here, we engineered probiotic Saccharomyces boulardii to constitutively secrete a single tetra-specific antibody that potently and broadly neutralized both toxins and demonstrated protection against primary and recurrent CDI in both prophylactic and therapeutic mouse models of disease. This yeast immunotherapy is orally administered, can be used concurrently with antibiotics, and may have potential as a prophylactic against CDI risk and as a therapeutic for patients with CDI.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Figures


References
-
- Kelly CP, LaMont JT, Clostridium difficile—More difficult than ever. N. Engl. J. Med 359, 1932–1940 (2008). - PubMed
-
- Lessa FC, Mu Y, Bamberg WM, Beldavs ZG, Dumyati GK, Dunn JR, Farley MM, Holzbauer SM, Meek JI, Phipps EC, Wilson LE, Winston LG, Cohen JA, Limbago BM, Fridkin SK, Gerding DN, McDonald LC, Burden of Clostridium difficile infection in the United States. N. Engl. J. Med 372, 825–834 (2015). - PMC - PubMed
-
- Kelly CP, Can we identify patients at high risk of recurrent Clostridium difficile infection? Clin. Microbiol. Infect 18 (suppl. 6), 21–27 (2012). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
