

ACE2 localizes to the respiratory cilia and is not increased by ACE inhibitors or ARBs
- PMID: 33116139
- PMCID: PMC7595232
- DOI: 10.1038/s41467-020-19145-6
ACE2 localizes to the respiratory cilia and is not increased by ACE inhibitors or ARBs
Abstract
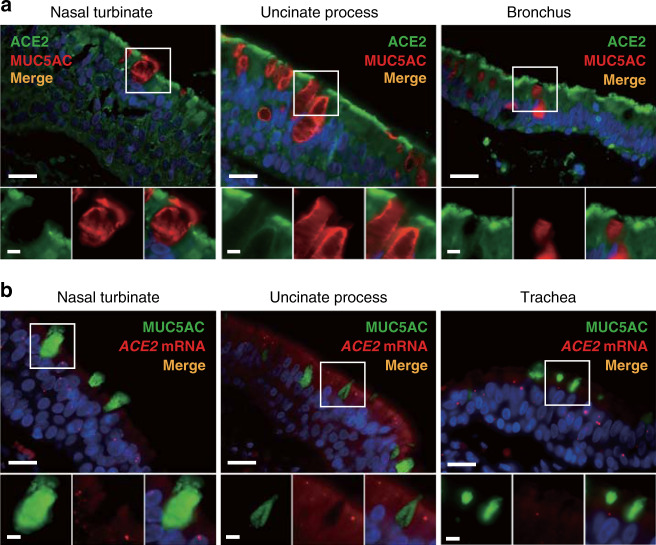
The coronavirus SARS-CoV-2 is the causative agent of the ongoing severe acute respiratory disease pandemic COVID-19. Tissue and cellular tropism is one key to understanding the pathogenesis of SARS-CoV-2. We investigate the expression and subcellular localization of the SARS-CoV-2 receptor, angiotensin-converting enzyme 2 (ACE2), within the upper (nasal) and lower (pulmonary) respiratory tracts of human donors using a diverse panel of banked tissues. Here, we report our discovery that the ACE2 receptor protein robustly localizes within the motile cilia of airway epithelial cells, which likely represents the initial or early subcellular site of SARS-CoV-2 viral entry during host respiratory transmission. We further determine whether ciliary ACE2 expression in the upper airway is influenced by patient demographics, clinical characteristics, comorbidities, or medication use, and show the first mechanistic evidence that the use of angiotensin-converting enzyme inhibitors (ACEI) or angiotensin II receptor blockers (ARBs) does not increase susceptibility to SARS-CoV-2 infection through enhancing the expression of ciliary ACE2 receptor. These findings are crucial to our understanding of the transmission of SARS-CoV-2 for prevention and control of this virulent pathogen.
Conflict of interest statement
The authors declare no competing interests.
Figures






Update of
-
Robust ACE2 protein expression localizes to the motile cilia of the respiratory tract epithelia and is not increased by ACE inhibitors or angiotensin receptor blockers.medRxiv [Preprint]. 2020 May 12:2020.05.08.20092866. doi: 10.1101/2020.05.08.20092866. medRxiv. 2020. Update in: Nat Commun. 2020 Oct 28;11(1):5453. doi: 10.1038/s41467-020-19145-6. PMID: 32511516 Free PMC article. Updated. Preprint.
References
-
- CDC COVID-19 Response Team. et al. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019 - United States, February 12-March 28, 2020. MMWR Morb. Mortal. Wkly Rep. 2020;69:382–386. doi: 10.15585/mmwr.mm6913e2. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
