

Efficacy and Safety of the CFTR Potentiator Icenticaftor (QBW251) in COPD: Results from a Phase 2 Randomized Trial
- PMID: 33116455
- PMCID: PMC7547289
- DOI: 10.2147/COPD.S257474
Efficacy and Safety of the CFTR Potentiator Icenticaftor (QBW251) in COPD: Results from a Phase 2 Randomized Trial
Abstract
Rationale: Excess mucus plays a key role in COPD pathogenesis. Cigarette smoke-induced cystic fibrosis transmembrane conductance regulator (CFTR) dysfunction may contribute to disease pathogenesis by depleting airway surface liquid and reducing mucociliary transport; these defects can be corrected in vitro by potentiating CFTR.
Objective: To assess the efficacy of the CFTR potentiator icenticaftor in improving airflow obstruction in COPD patients with symptoms of chronic bronchitis.
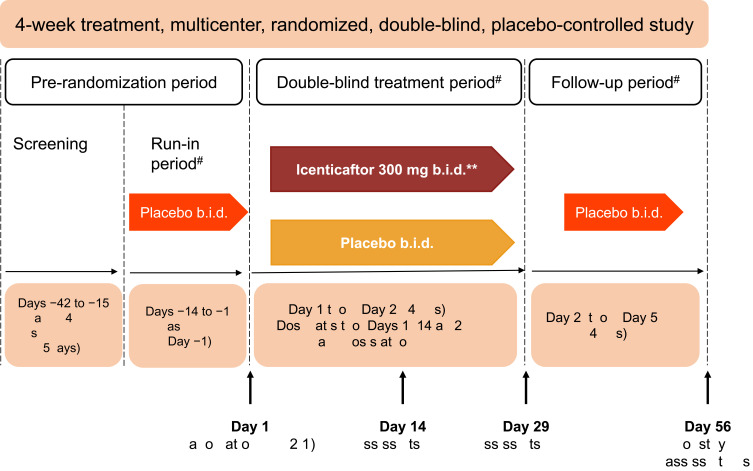
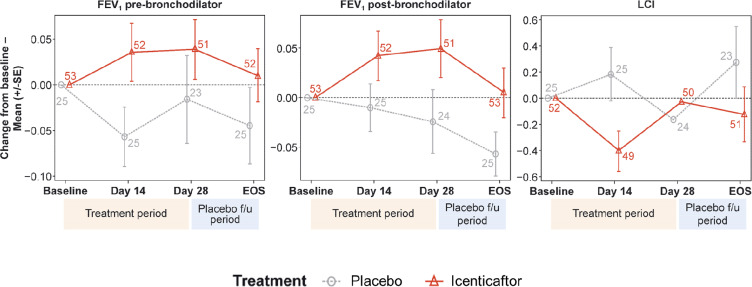
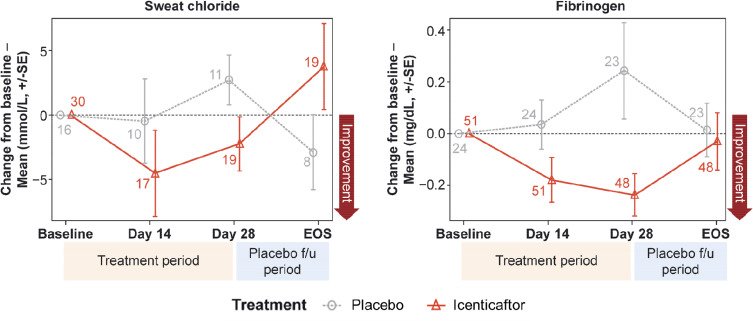
Methods: In this double-blind, placebo-controlled study, COPD patients were randomized (2:1) to either icenticaftor 300 mg or placebo b.i.d. This non-confirmatory proof of concept study was powered for lung clearance index (LCI) and pre-bronchodilator FEV1, with an estimated sample size of 90 patients. The primary endpoint was change from baseline in LCI for icenticaftor versus placebo at Day 29; key secondary endpoints included change from baseline in pre- and post-bronchodilator FEV1 on Day 29. Key exploratory endpoints included change from baseline in sweat chloride, plasma fibrinogen levels, and sputum colonization.
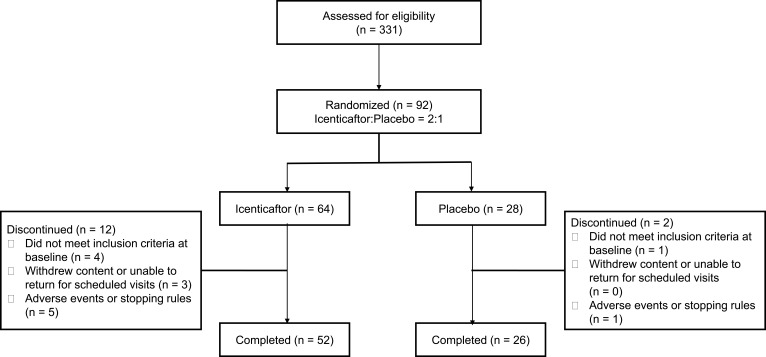
Results: Ninety-two patients were randomized (icenticaftor, n=64; placebo, n=28). At Day 29, icenticaftor showed no improvement in change in LCI (treatment difference: 0.28 [19% probability of being better than placebo]), an improvement in pre-bronchodilator FEV1 (mean: 50 mL [84% probability]) and an improvement in post-bronchodilator FEV1 (mean: 63 mL [91% probability]) over placebo. Improvements in sweat chloride, fibrinogen and sputum bacterial colonization were also observed. Icenticaftor was safe and well tolerated.
Conclusion: The CFTR potentiator icenticaftor increased FEV1 versus placebo after 28 days and was associated with improvements in systemic inflammation and sputum bacterial colonization in COPD patients; no improvements in LCI with icenticaftor were observed.
Keywords: CFTR potentiator; chronic bronchitis; chronic obstructive pulmonary disease; cystic fibrosis transmembrane conductance regulator potentiator; icenticaftor; QBW251; mucociliary clearance.
© 2020 Rowe et al.
Conflict of interest statement
Steven M Rowe reports grants and personal fees from Novartis during the conduct of the study; grants and personal fees from Bayer, grants from Translate Bio, grants from Proteostasis, grants, personal fees and non-financial support from Galapagos/Abbvie, grants, personal fees and in kind support for research from Synedgen/Synspira, grants from Eloxx, grants and personal fees from Celtaxsys, grants, personal fees, non-financial support from Vertex Pharmaceuticals Inc, grants, personal fees and stock options from Renovion, grants and personal fees from Arrowhead, grants, personal fees and in kind support for research from Ionis, grants from AstraZeneca, grants from N30/Nivalis, grants from PTC Therapeutics, personal fees from Genentech, personal fees, non-financial support from Boehringer Ingelheim, grants from Janssen, Vivus, Actelion, Johnson and Johnson, and other related entities, outside the submitted work. Mark T Dransfield reports grants from the NIH, Department of Defense and American Lung Association; consulting fees from AstraZeneca, GlaxoSmithKline, Mereo, Quark and Teva; travel support from Pulmonx; and contracted clinical trial support from AstraZeneca, Boehringer Ingelheim, Boston Scientific, Gala, Nuvaira, PneumRx/BTG, Pulmonx and Yungjin. Ieuan Jones, Katy A Hayes, David J Rowlands and Sarah S Grant have patent 8247436 issued and are employees of Novartis. Nazmul Haque, Stephen Gleason and Denise P Yates are employees of Novartis. Kenneth Kulmatycki have a patent issued and is an employee of Novartis. Martin Gosling was an employee of Novartis between 2001 and 2014. He is now affiliated with Enterprise Therapeutics. Henry Danahay was an employee of Novartis between 1997 and 2014. He is now affiliated with Enterprise Therapeutics. The authors report no other conflicts of interest in this work.
Figures
References
-
- Global initiative for chronic obstructive lung disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2018 Report); 2018. - PubMed
-
- World health organization. Chronic Obstructive Pulmonary Disease (Copd); 2016.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
