

Cost-Effectiveness of Cardiac Resynchronization Therapy in Patients with Heart Failure in Thailand
- PMID: 33116697
- PMCID: PMC7569046
- DOI: 10.2147/CEOR.S268553
Cost-Effectiveness of Cardiac Resynchronization Therapy in Patients with Heart Failure in Thailand
Abstract
Background: Cardiac resynchronization therapy (CRT) improves symptoms and survival in patients with heart failure (HF). However, the CRT devices are costly and can impose a significant burden to the relatively constrained health budgets of middle-income countries such as Thailand. The aim of this study was to analyze the cost-effectiveness of CRT in combination with optimal medical therapy (OMT) relative to patients with OMT alone.
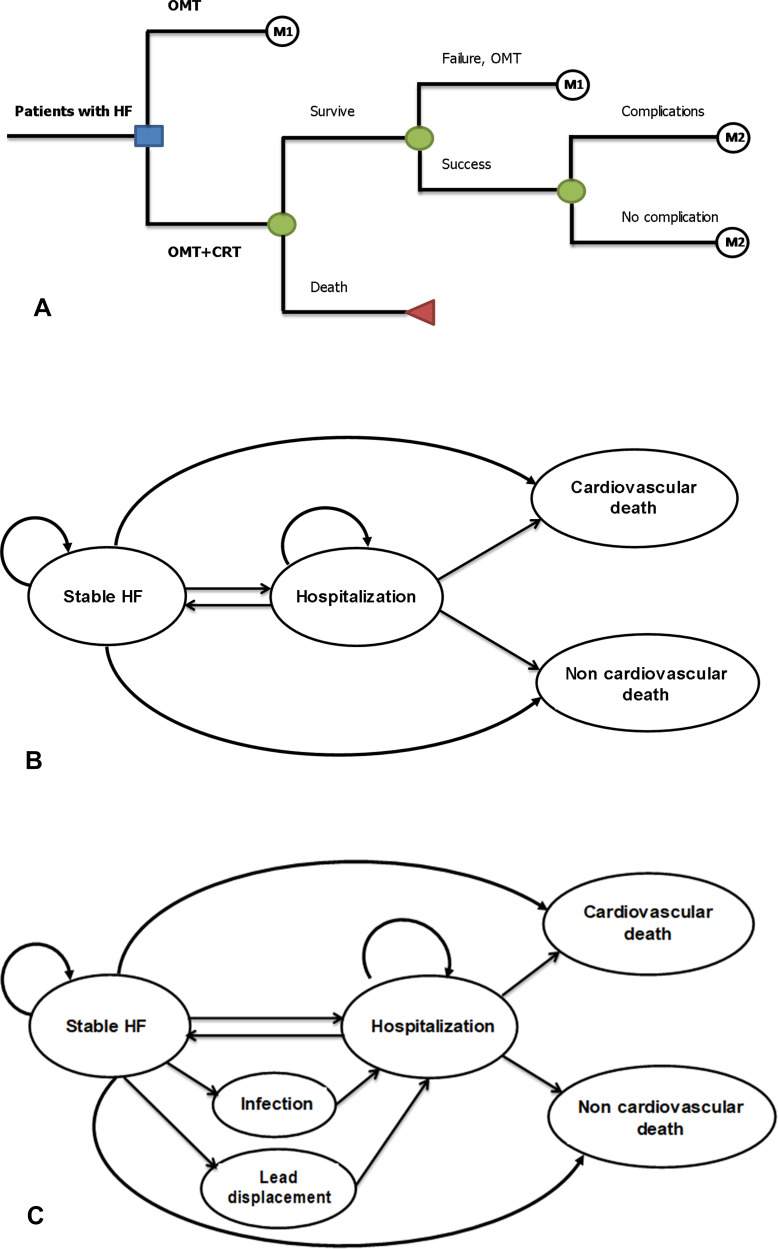
Methods: A two-component model was used to analyze lifetime costs and quality-adjusted life-years (QALYs) from a healthcare perspective. Clinical inputs were mostly obtained from meta-analysis of landmark trials. All cost-related data, risk of non-cardiovascular death and readmission rate were based on Thai HF data. Costs and QALYs were discounted at 3%. Findings were reported as an incremental cost-effectiveness ratio (ICER). A variety of sensitivity analyses were also performed.
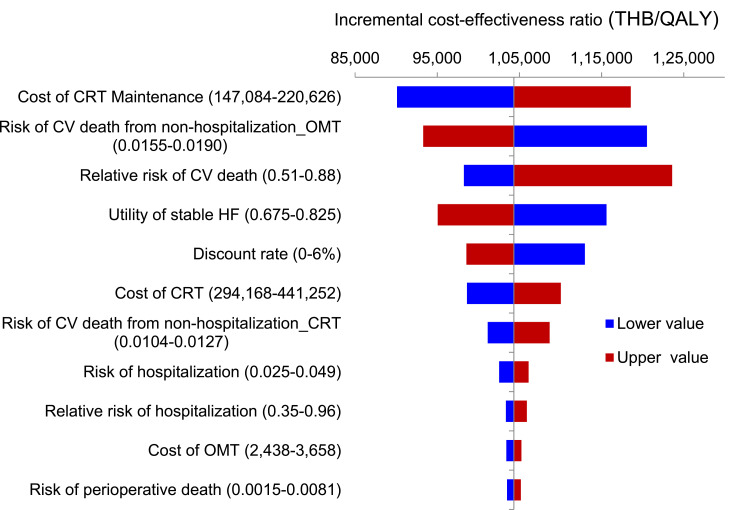
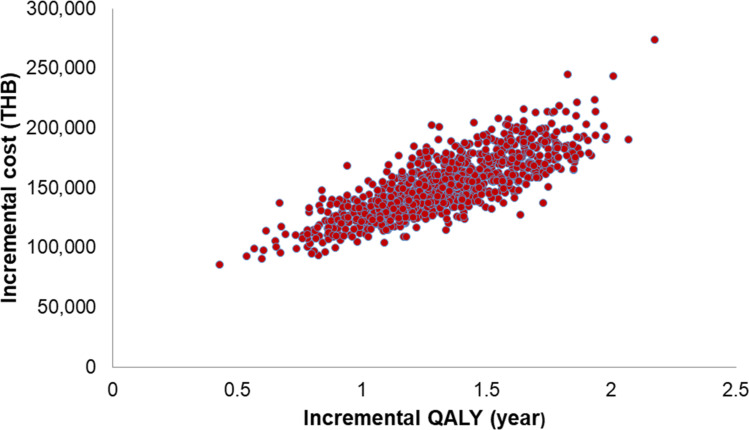
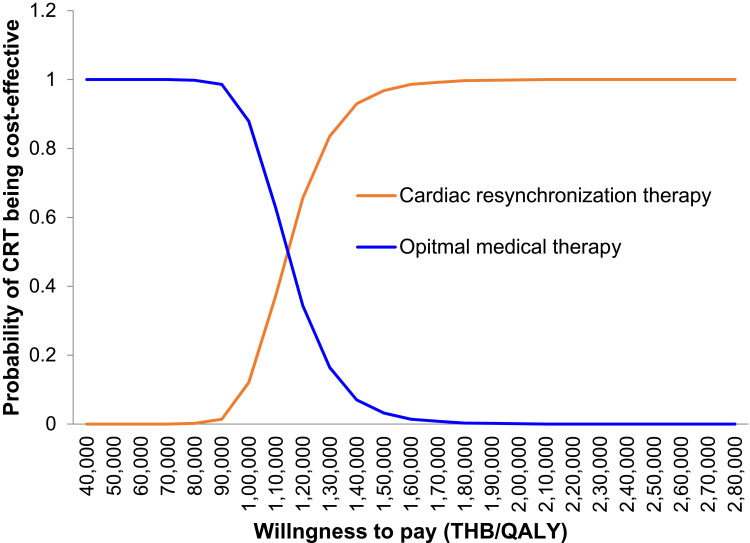
Results: CRT plus OMT costs more than OMT (123,279 vs 11,165 THB or 3,972.90 vs 359.81 USD), and is more effective (3.57 QALYs vs 2.49 QALYs), yielding an ICER of 104,325 THB per QALY (3,362.07 USD per QALY). CRT was cost-effective at the Thai willingness to pay threshold of 160,000 THB per QALY (5,156.30 USD per QALY). The results were sensitive to cost of CRT maintenance.
Conclusion: The use of CRT was associated with a cost-effectiveness ratio below generally accepted benchmarks for therapeutic interventions of 160,000 THB per QALY (5,156.30 USD per QALY). This suggests that the clinical benefits of CRT can be achieved at a reasonable cost in Thai HF patients.
Keywords: Thailand; cardiac resynchronization therapy; cost-effectiveness; heart failure; quality-adjusted life-years.
© 2020 Permsuwan et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics-2016 update: a report from the American heart association. Circulation. 2016;133(4):e38–360. - PubMed
-
- Summary report of morbidity A.D.2015. Bureau of policy and strategy MoP, editor. Bangkok: Samcharoen Panich; 2016.
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
