

Neuro-Endovascular Intervention in Traumatic Carotico-Cavernous Fistulae: A Single-Center Experience
- PMID: 33116784
- PMCID: PMC7585868
- DOI: 10.2147/IJGM.S273603
Neuro-Endovascular Intervention in Traumatic Carotico-Cavernous Fistulae: A Single-Center Experience
Abstract
Introduction: The aim of this research was to describe a single-center practical experience in the management of traumatic carotid cavernous fistula (CCF).
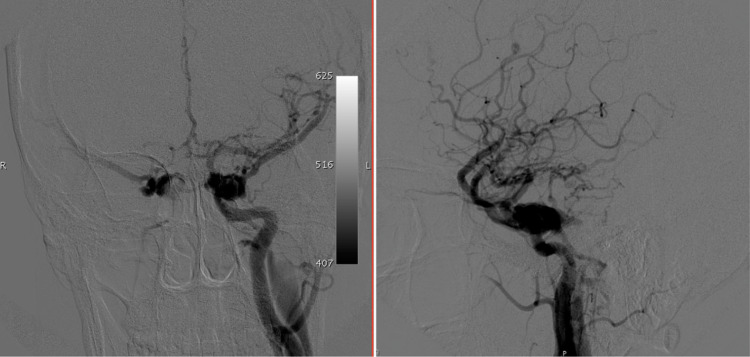
Methods: There were a total of 31 patients between January 2005 and December 2019 with post-traumatic carotid cavernous sinus fistula (tCCF) who underwent treatment. We classified them into 2 types according to the flow of the CCF: patients with high flow CCF and patients with low flow CCF.
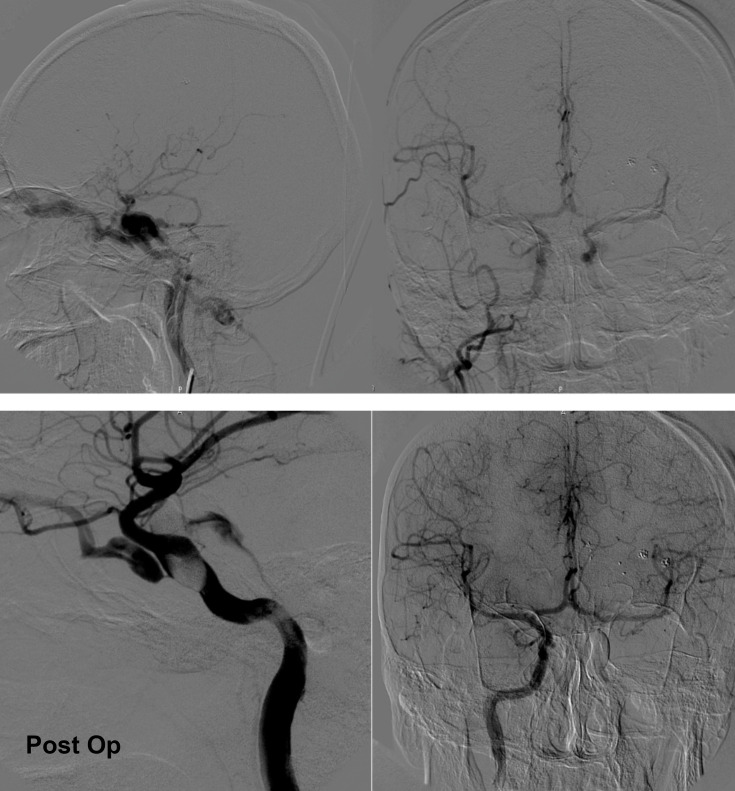
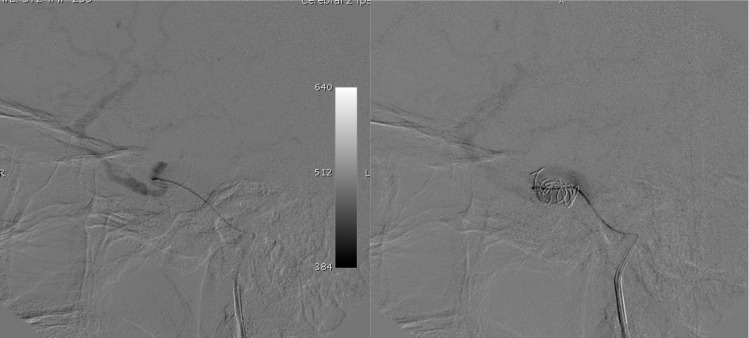
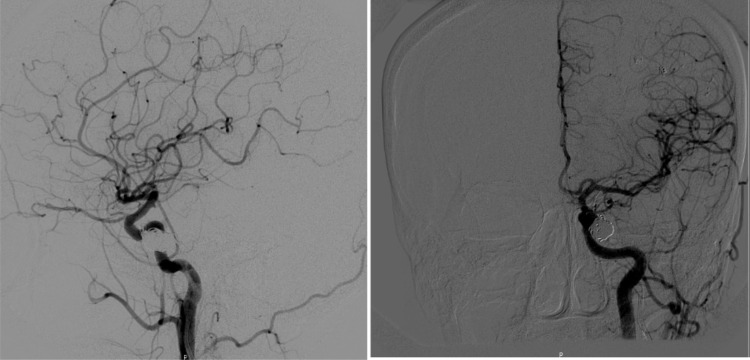
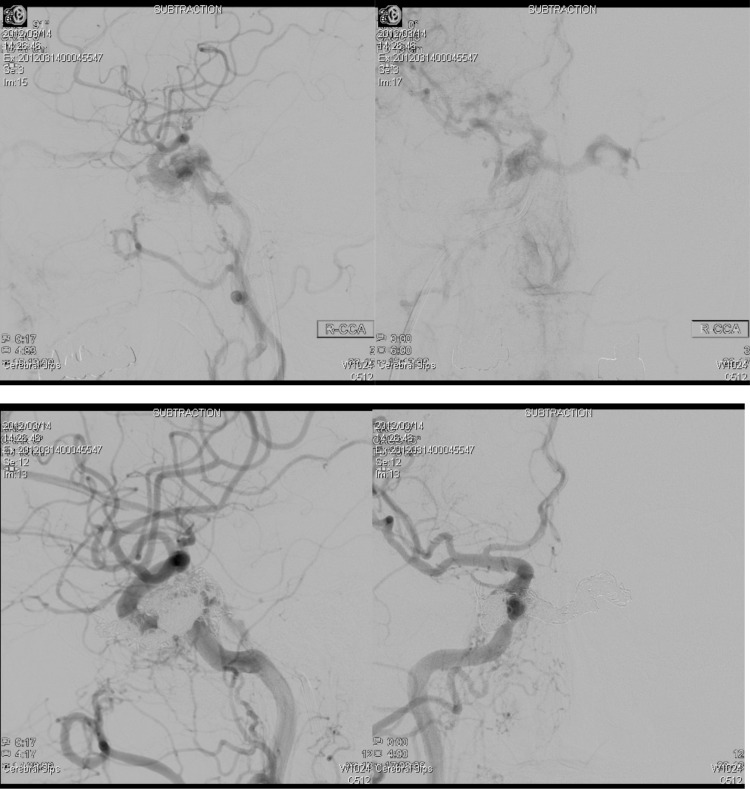
Results: Angiography revealed the high flow types on 21 patients (67.7%), the mean of patients ages are 31.5 years. Onyx embolization was performed in 1 patient (4.76%), transarterial balloon embolization was carried out in 10 patients (47.61%), transarterial coiling in 3 (14.28%) patients while 5 (28.8%) patients underwent transvenous routes to insert the coil and 2 patients (9.52%) were treated conservatively. Complete occlusion was achieved on all patients with coiling whereas the other treatment experiences the reducing flow of the fistula. We obtained 10 patients (32.2%) with a mean of 40.3 years as low flow type CCF. The patients with the low flow type mostly treated conservatively, because their symptoms were acceptable and intermittent.
Conclusion: The ballooning currently became the more affordable treatment in our center. Balloon embolization was recommended for medium- and large-size fistula. The coils should be recommended for small-size fistula. In some cases occlusion of the fistula cannot be obtained using the detachable balloon, a coil can be used to occlude the cavernous sinus via trans arterial or trans venous access. If the fistula failed to be treated in traditional ways using balloons or coils, occlusion of the parent vessels could be another option.
Keywords: angiography; carotid cavernous sinus fistula; embolization; transarterial; transvenous; trauma.
© 2020 Thohar Arifin et al.
Conflict of interest statement
The authors report no conflicts of interest for this work.
Figures

References
-
- Pashapour A, Mohammadian R, Salehpour F, et al. Long-term endovascular treatment outcome of 46 patients with cavernous sinus dural arteriovenous fistulas presenting with ophthalmic symptoms. A non-controlled trial with clinical and angiographic follow-up. Neuroradiol J. 2014;27(4):461–470. doi: 10.15274/NRJ-2014-10079 - DOI - PMC - PubMed
-
- Andrade G, Ponte de Souza MLP, Marques R, Silva JL, Abath C, Azevedo-Filho HRC. Endovascular treatment of traumatic carotid cavernous fistula with balloon-assisted sinus coiling. A technical description and initial results. Interv Neuroradiol. 2013;19(4):445–454. doi: 10.1177/159101991301900407 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
