

Testicular Torsion in the Emergency Room: A Review of Detection and Management Strategies
- PMID: 33116959
- PMCID: PMC7567548
- DOI: 10.2147/OAEM.S236767
Testicular Torsion in the Emergency Room: A Review of Detection and Management Strategies
Abstract
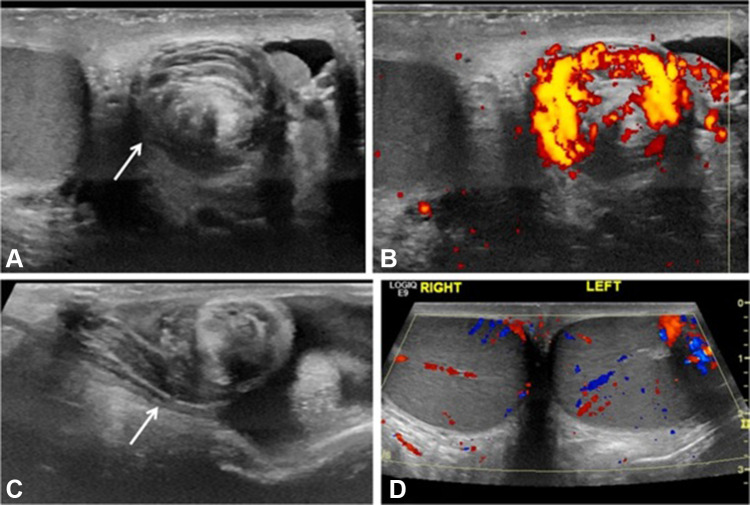
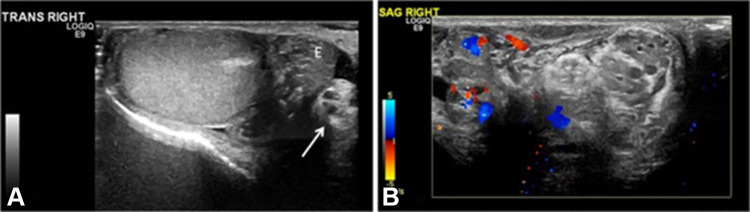
Testicular torsion is a challenging and time-sensitive diagnosis that is encountered frequently in daily practice, especially in the emergency room. A thorough history, the presence of a painful and swollen testis and testicular ultrasonography plays a vital role in the prompt diagnosis of testicular torsion. Prompt diagnosis is essential to prevent complications of testicular torsion which include testicular infarction, necrosis, and sub/infertility. This can be challenging as there are various other conditions that may mimic the presentation of testicular torsion. Since testicular torsion is an extremely time-sensitive diagnosis, it may also be a subject of many medicolegal challenges. This review article serves as a guide for clinicians involved with the diagnosis and management of testicular torsion. We review and discuss detection and management strategies based on their validity, statistical significance, and effectiveness in enabling prompt diagnosis and management of testicular torsion. Medicolegal implications of testicular torsion are also highlighted.
Keywords: acute scrotum; emergency room; orchidectomy; scrotal pain; testis torsion.
© 2020 Laher et al.
Conflict of interest statement
The authors hereby certify that all authors are free from any financial or other conflicts of interest for this work.
Figures

References
-
- Ogunyemi OI. Testicular Torsion; Published 2018. Available from: https://emedicine.medscape.com/article/2036003-overview#a7. Accessed February17, 2020.
-
- Sharp VJ, Kieran K, Arlen AM. Testicular torsion: diagnosis, evaluation, and management. Am Fam Physician. 2013;88(12):835–840. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
