

Current Understanding of Circulating Biomarkers in Pulmonary Hypertension Due to Left Heart Disease
- PMID: 33117832
- PMCID: PMC7575769
- DOI: 10.3389/fmed.2020.570016
Current Understanding of Circulating Biomarkers in Pulmonary Hypertension Due to Left Heart Disease
Abstract
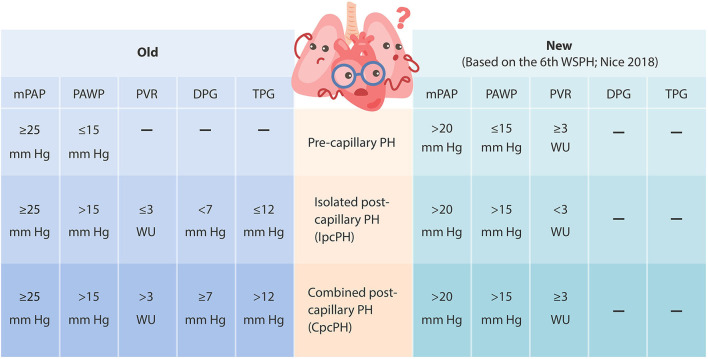
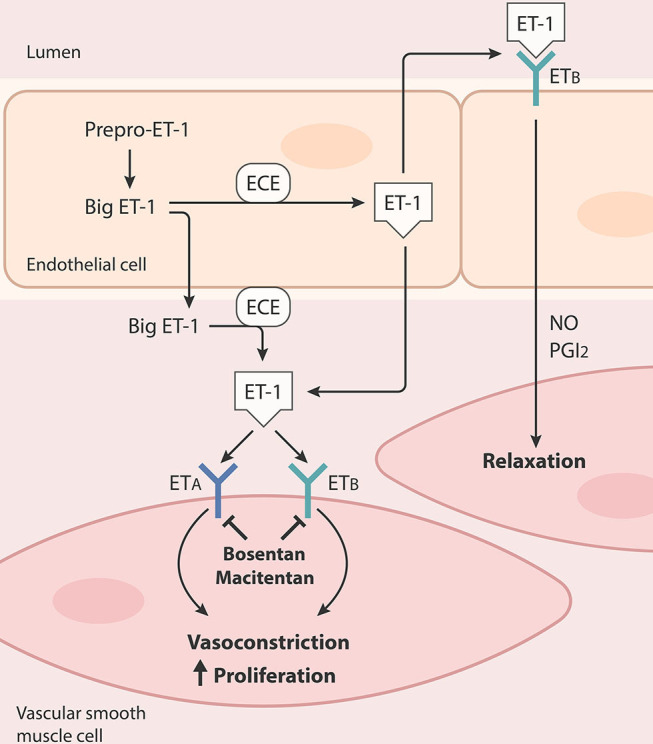
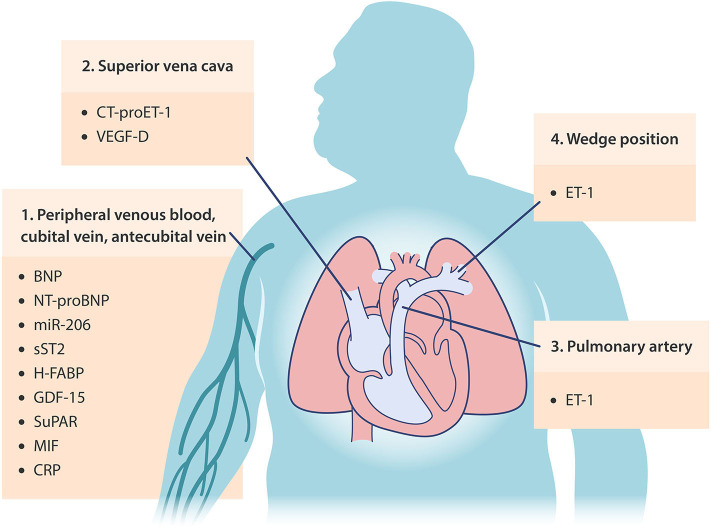
Pulmonary hypertension due to left heart disease (PH-LHD; Group 2), especially in the setting of heart failure with preserved ejection fraction (HFpEF), is the most frequent cause of PH. Despite its prevalence, no effective therapies for PH-LHD are available at present. This is largely due to the lack of a concise definition for hemodynamic phenotyping, existence of significant gaps in the understanding of the underlying pathology and the impact of associated comorbidities, as well as the absence of specific biomarkers that can aid in the early diagnosis and management of this challenging syndrome. Currently, B-type natriuretic peptide (BNP) and N-terminal proBNP (NT-proBNP) are guideline-recommended biomarkers for the diagnosis and prognosis of heart failure (HF) and PH. Endothelin-1 (ET-1), vascular endothelial growth factor-D (VEGF-D), and microRNA-206 have also been recently identified as new potential circulating biomarkers for patients with PH-LHD. In this review, we aim to present the current state of knowledge of circulating biomarkers that can be used to guide future research toward diagnosis, refine specific patient phenotype, and develop therapeutic approaches for PH-LHD, with a particular focus on PH-HFpEF. Potential circulating biomarkers identified in pre-clinical models of PH-LHD are also summarized here.
Keywords: HFpEF - heart failure with preserved ejection fraction; PH-HFpEF; biomarkers; group 2 PH; pulmonary hypertension.
Copyright © 2020 Todd and Lai.
Figures
Similar articles
-
Renal function, N-terminal Pro-B-Type natriuretic peptide, propeptide big-endothelin and patients with heart failure and preserved ejection fraction.Peptides. 2019 Jan;111:112-117. doi: 10.1016/j.peptides.2018.04.003. Epub 2018 Apr 21. Peptides. 2019. PMID: 29684593
-
Left heart disease: a frequent cause of early pulmonary hypertension in systemic sclerosis, unrelated to elevated NT-proBNP levels or overt cardiac fibrosis but associated with increased levels of MR-proANP and MR-proADM: retrospective analysis of a French Canadian cohort.Scand J Rheumatol. 2014;43(4):314-23. doi: 10.3109/03009742.2013.854407. Epub 2014 Feb 6. Scand J Rheumatol. 2014. PMID: 25089008
-
Management of Pulmonary Hypertension in Left Heart Disease.Methodist Debakey Cardiovasc J. 2021 Jul 1;17(2):115-123. doi: 10.14797/RKQN5397. eCollection 2021. Methodist Debakey Cardiovasc J. 2021. PMID: 34326931 Free PMC article.
-
Considerations in the Diagnosis and Management of Pulmonary Hypertension Associated With Left Heart Disease.JACC Heart Fail. 2024 Aug;12(8):1328-1342. doi: 10.1016/j.jchf.2024.04.031. Epub 2024 Jul 3. JACC Heart Fail. 2024. PMID: 38970588 Review.
-
Pulmonary Hypertension in Heart Failure.Int J Heart Fail. 2021 Apr 21;3(3):147-159. doi: 10.36628/ijhf.2020.0053. eCollection 2021 Jul. Int J Heart Fail. 2021. PMID: 36262642 Free PMC article. Review.
Cited by
-
Prevalence of aortic stenosis and TAVR outcomes in patients with systemic sclerosis-associated pulmonary hypertension.Pulm Circ. 2022 Jul 1;12(3):e12118. doi: 10.1002/pul2.12118. eCollection 2022 Jul. Pulm Circ. 2022. PMID: 36034401 Free PMC article.
-
Plasma Proteomics Identifies B2M as a Regulator of Pulmonary Hypertension in Heart Failure With Preserved Ejection Fraction.Arterioscler Thromb Vasc Biol. 2024 Jul;44(7):1570-1583. doi: 10.1161/ATVBAHA.123.320270. Epub 2024 May 30. Arterioscler Thromb Vasc Biol. 2024. PMID: 38813697 Free PMC article.
-
Severe Aortic Valve Stenosis and Pulmonary Hypertension: A Systematic Review of Non-Invasive Ways of Risk Stratification, Especially in Patients Undergoing Transcatheter Aortic Valve Replacement.J Pers Med. 2022 Apr 8;12(4):603. doi: 10.3390/jpm12040603. J Pers Med. 2022. PMID: 35455719 Free PMC article. Review.
-
Integrative Analyses of Circulating Proteins and Metabolites Reveal Sex Differences in the Associations with Cardiac Function among DCM Patients.Int J Mol Sci. 2024 Jun 21;25(13):6827. doi: 10.3390/ijms25136827. Int J Mol Sci. 2024. PMID: 38999939 Free PMC article.
-
Plasma tumour necrosis factor-alpha-related proteins in prognosis of heart failure with pulmonary hypertension.ESC Heart Fail. 2023 Dec;10(6):3582-3591. doi: 10.1002/ehf2.14507. Epub 2023 Sep 29. ESC Heart Fail. 2023. PMID: 37772417 Free PMC article.
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous