

Management of Acute Mesenteric Venous Thrombosis: A Systematic Review of Contemporary Studies
- PMID: 33118463
- PMCID: PMC8258716
- DOI: 10.1177/1457496920969084
Management of Acute Mesenteric Venous Thrombosis: A Systematic Review of Contemporary Studies
Abstract
Background and aims: Acute mesenteric venous thrombosis accounts for up to 20% of all patients with acute mesenteric ischemia in high-income countries. Acute mesenteric venous thrombosis is nowadays relatively more often diagnosed with intravenous contrast-enhanced computed tomography in the portal phase than at explorative laparotomy No high-quality comparative studies between anticoagulation alone, endovascular therapy, or surgery exists. The aim of the present systematic review was to offer a contemporary overview on management.
Materials and methods: Eleven relevant published original studies with series of at least ten patients were retrieved from a Pub Med search between 2015 and 2020 using the Medical Subject Heading term "mesenteric venous thrombosis."
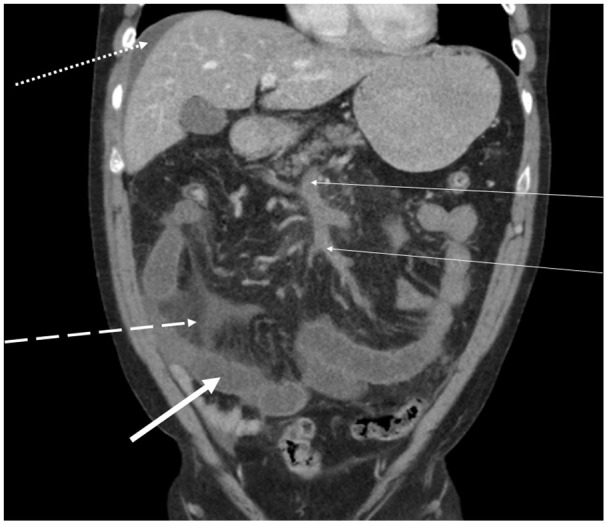
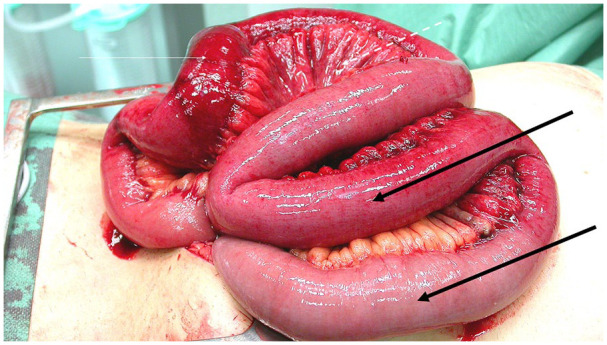
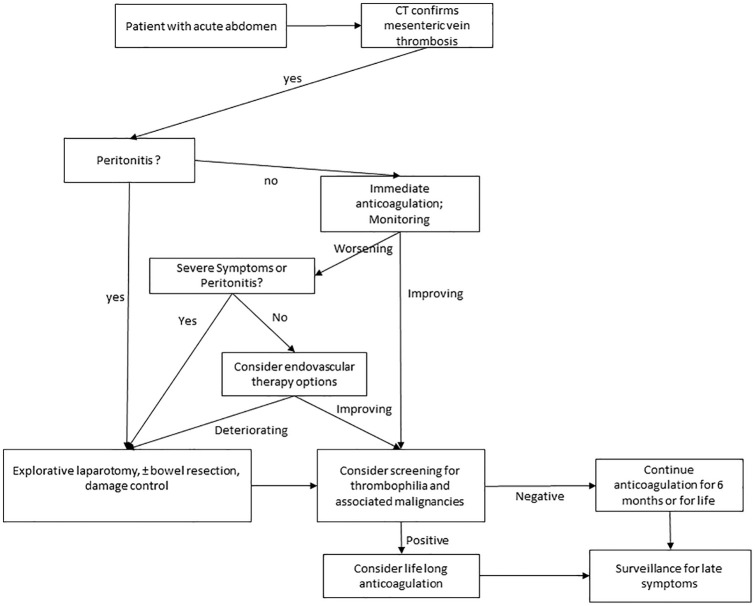
Results: When MVT is diagnosed early, immediate anticoagulation with either unfractionated heparin or subcutaneous low-molecular-weight heparin should commence. Surgeons need to be aware of the importance to scrutinize the computed tomography images themselves for assessment of secondary intestinal abnormalities to mesenteric venous thrombosis and the risk of bowel resection and worse prognosis. Progression toward peritonitis is an indication for explorative laparotomy and assessment of bowel viability. Frank transmural small bowel necrosis should be resected and bowel anastomosis may be delayed for several days until second look. Meanwhile, intravenous full-dose unfractionated heparin should be given at the end of the first operation. Postoperative major intra-abdominal or gastrointestinal bleeding occurs rarely, but the heparin effect can instantaneously be reversed by protamine sulfate. Patients who do not improve during conservative therapy with anticoagulation alone but without developing peritonitis may be subjected to endovascular therapy in expert centers. When the patient's intestinal function has recovered, with or without bowel resection, switch from parenteral unfractionated heparin or low-molecular-weight heparin therapy to oral anticoagulation can be performed. There is a trend that direct oral anticoagulants are increasingly used instead of vitamin K antagonists. Up to now, direct oral anticoagulants have been shown to be equally effective with the same rate of bleeding complications. Patients with no strong permanent trigger factor for mesenteric venous thrombosis such as intra-abdominal cancer should undergo blood screening for inherited and acquired thrombophilia.
Conclusion: Early diagnosis with emergency computed tomography with intravenous contrast-enhancement and imaging in the portal phase and anticoagulation therapy is necessary to be able to have a succesful non-operative succesful course.
Keywords: Acute care surgery and trauma; anticoagulation; intestinal ischemia; management; mesenteric venous thrombosis; vascular surgery.
Conflict of interest statement
Figures

References
-
- Acosta S: Epidemiology of mesenteric vascular disease: Clinical implications. Semin Vasc Surg 2010;23:4–8. - PubMed
-
- Zarrouk M, Salim S, Elf J, et al.: Testing for thrombophilia in mesenteric venous thrombosis: Retrospective original study and systematic review. Best Pract Res Clin Gastroenterol 2017;31:39–48. - PubMed
-
- McKinsey JF, Gewertz BL: Acute mesenteric ischemia. Surg Clin North Am 1997;77:307–318. - PubMed
-
- Salim S, Ekberg O, Elf J, et al.: Clinical implications of CT findings in mesenteric venous thrombosis at admission. Emerg Radiol 2018;25:407–413. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
