

Myocardial Gene Expression Signatures in Human Heart Failure With Preserved Ejection Fraction
- PMID: 33118835
- PMCID: PMC7856095
- DOI: 10.1161/CIRCULATIONAHA.120.050498
Myocardial Gene Expression Signatures in Human Heart Failure With Preserved Ejection Fraction
Erratum in
-
Correction to: Myocardial Gene Expression Signatures in Human Heart Failure With Preserved Ejection Fraction.Circulation. 2021 Jun 8;143(23):e1027. doi: 10.1161/CIR.0000000000000990. Epub 2021 Jun 7. Circulation. 2021. PMID: 34097457 No abstract available.
Abstract
Background: Heart failure (HF) with preserved ejection fraction (HFpEF) constitutes half of all HF but lacks effective therapy. Understanding of its myocardial biology remains limited because of a paucity of heart tissue molecular analysis.
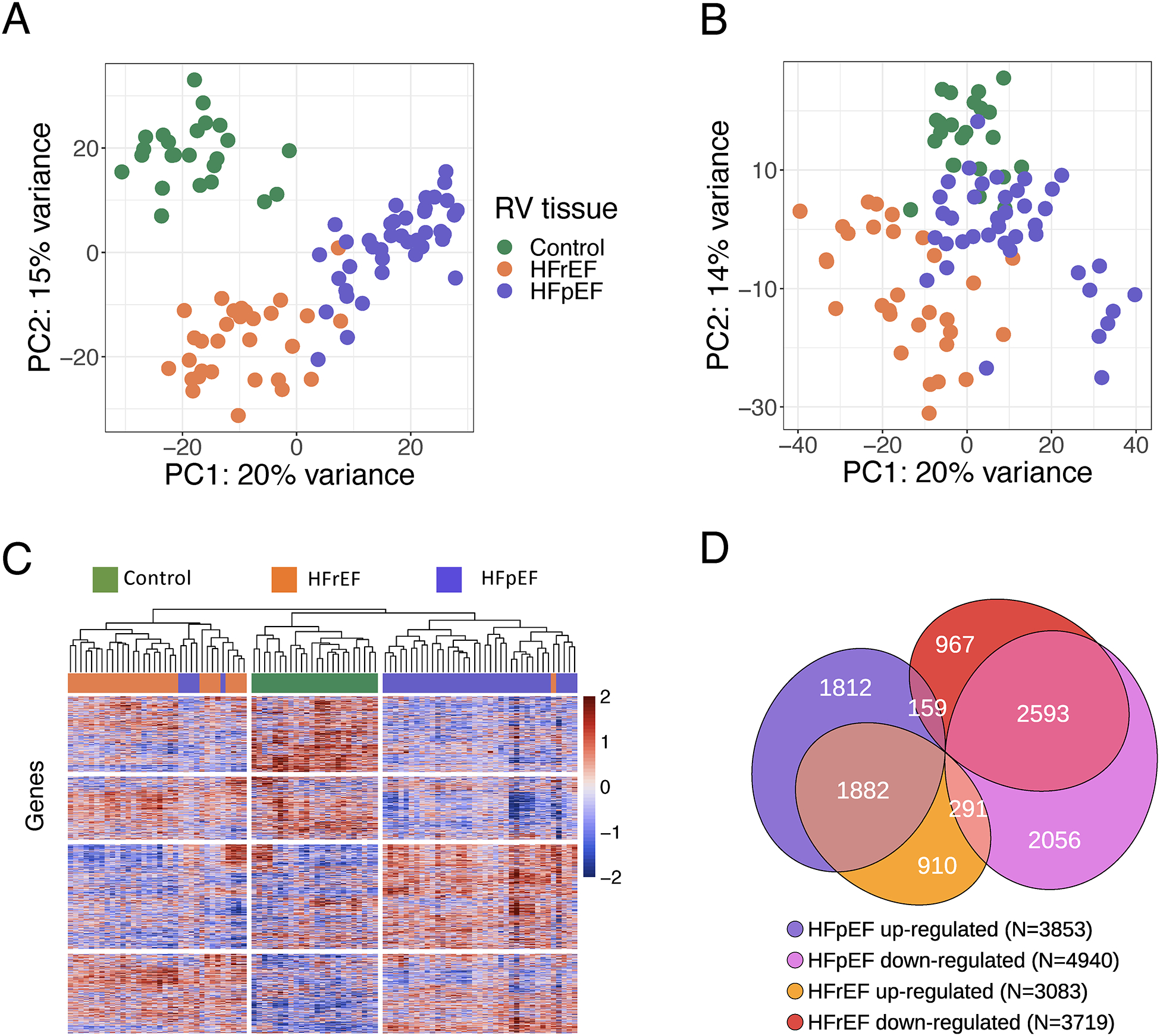
Methods: We performed RNA sequencing on right ventricular septal endomyocardial biopsies prospectively obtained from patients meeting consensus criteria for HFpEF (n=41) contrasted with right ventricular septal tissue from patients with HF with reduced ejection fraction (HFrEF, n=30) and donor controls (n=24). Principal component analysis and hierarchical clustering tested for transcriptomic distinctiveness between groups, effect of comorbidities, and differential gene expression with pathway enrichment contrasted HF groups and donor controls. Within HFpEF, non-negative matrix factorization and weighted gene coexpression analysis identified molecular subgroups, and the resulting clusters were correlated with hemodynamic and clinical data.
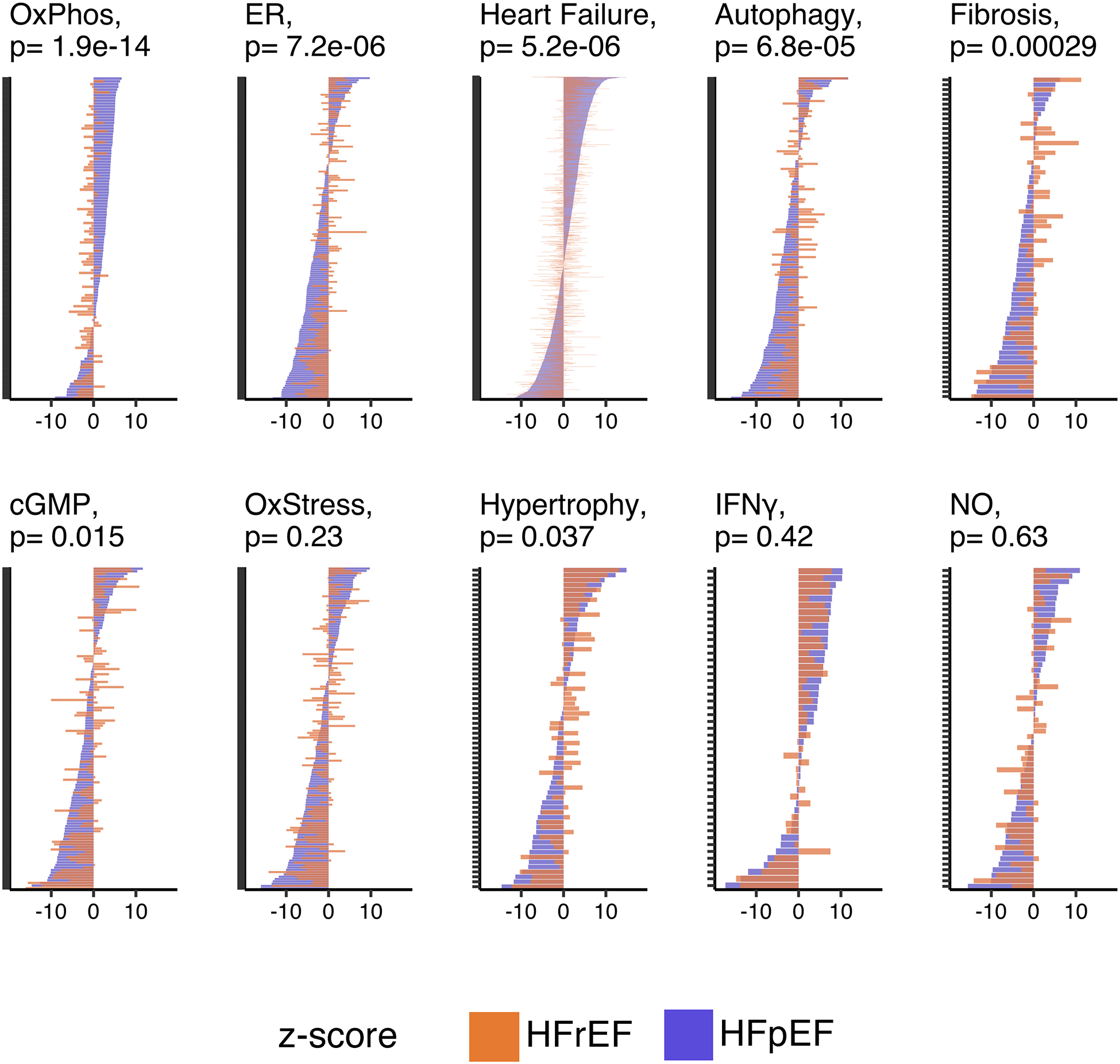
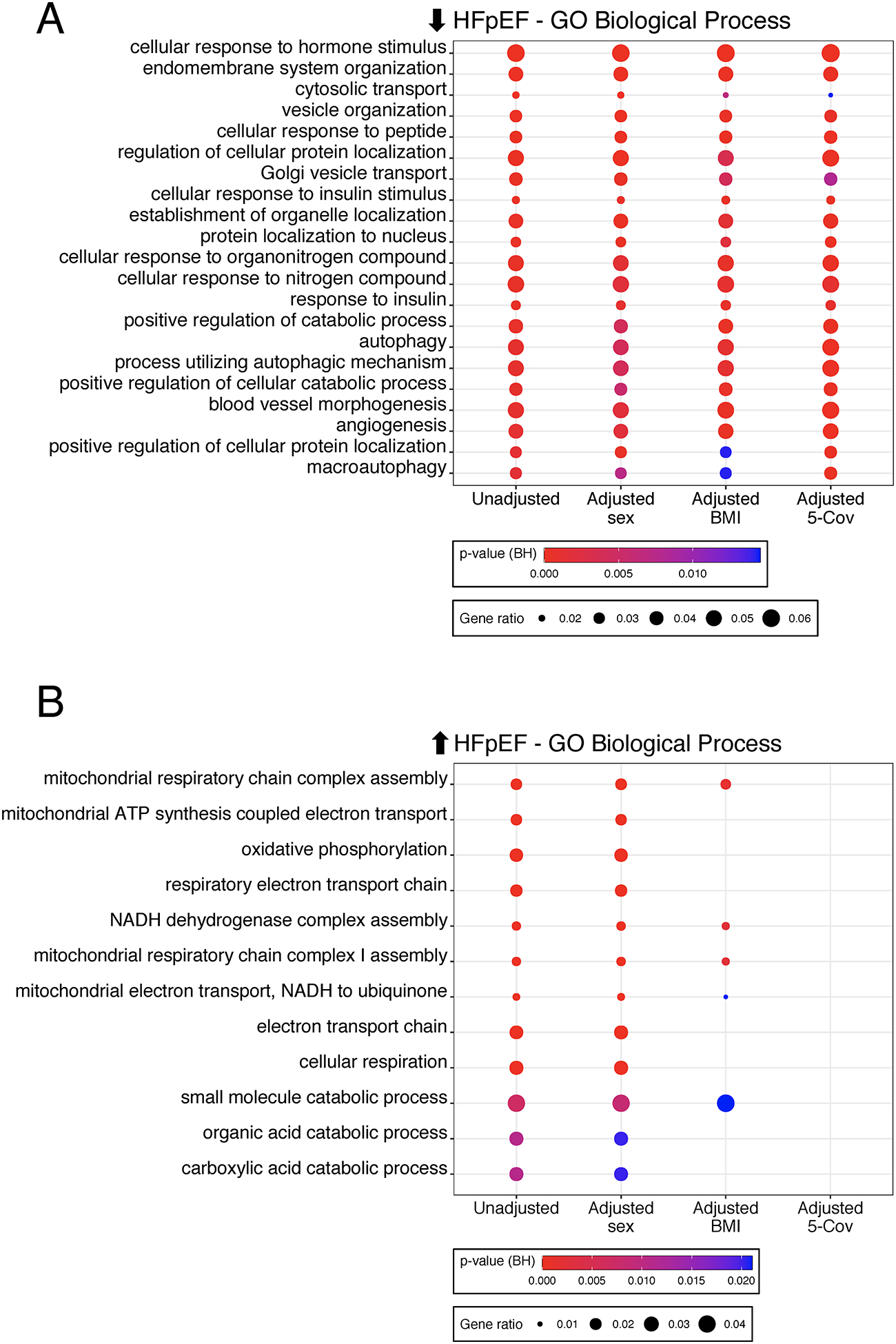
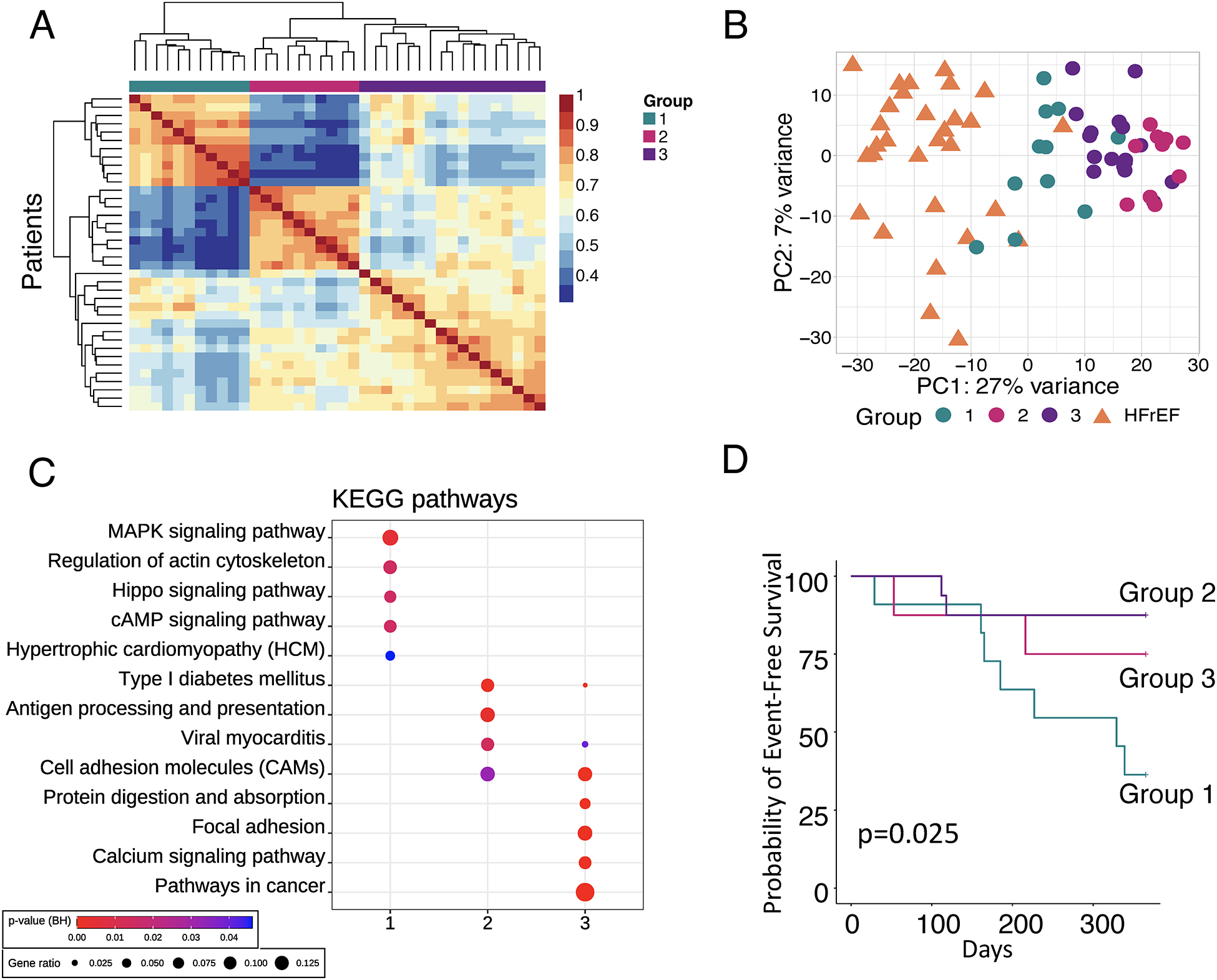
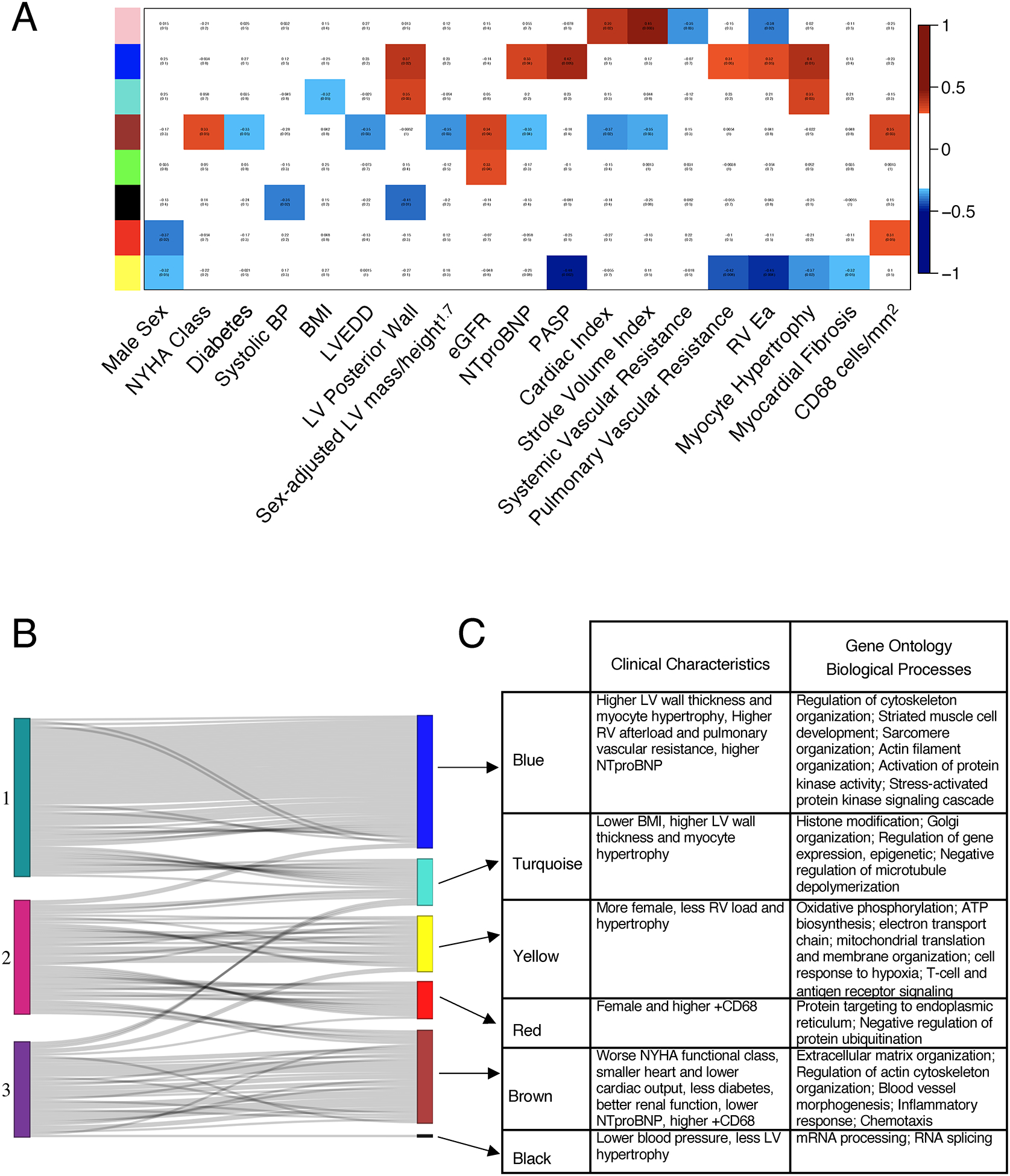
Results: Patients with HFpEF were more often women (59%), African American (68%), obese (median body mass index 41), and hypertensive (98%), with clinical HF characterized by 65% New York Heart Association Class III or IV, nearly all on a loop diuretic, and 70% with a HF hospitalization in the previous year. Principal component analysis separated HFpEF from HFrEF and donor controls with minimal overlap, and this persisted after adjusting for primary comorbidities: body mass index, sex, age, diabetes, and renal function. Hierarchical clustering confirmed group separation. Nearly half the significantly altered genes in HFpEF versus donor controls (1882 up, 2593 down) changed in the same direction in HFrEF; however, 5745 genes were uniquely altered between HF groups. Compared with controls, uniquely upregulated genes in HFpEF were enriched in mitochondrial adenosine triphosphate synthesis/electron transport, pathways downregulated in HFrEF. HFpEF-specific downregulated genes engaged endoplasmic reticulum stress, autophagy, and angiogenesis. Body mass index differences largely accounted for HFpEF upregulated genes, whereas neither this nor broader comorbidity adjustment altered pathways enriched in downregulated genes. Non-negative matrix factorization identified 3 HFpEF transcriptomic subgroups with distinctive pathways and clinical correlates, including a group closest to HFrEF with higher mortality, and a mostly female group with smaller hearts and proinflammatory signaling. These groupings remained after sex adjustment. Weighted gene coexpression analysis yielded analogous gene clusters and clinical groupings.
Conclusions: HFpEF exhibits distinctive broad transcriptomic signatures and molecular subgroupings with particular clinical features and outcomes. The data reveal new signaling targets to consider for precision therapeutics.
Keywords: computational biology; heart failure; humans; sequence analysis, RNA.
Figures
References
-
- Sharma K, Hill T, Grams M, Daya NR, Hays AG, Fine D, Thiemann DR, Weiss RG, Tedford RJ, Kass DA, et al. Outcomes and Worsening Renal Function in Patients Hospitalized With Heart Failure With Preserved Ejection Fraction. Am J Cardiol. 2015;116:1534–1540. doi: 10.1016/j.amjcard.2015.08.019 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
