

Predictors of Delayed Recognition of Critical Illness in Emergency Department Patients and Its Effect on Morbidity and Mortality
- PMID: 33118840
- PMCID: PMC8081733
- DOI: 10.1177/0885066620967901
Predictors of Delayed Recognition of Critical Illness in Emergency Department Patients and Its Effect on Morbidity and Mortality
Abstract
Purpose: Timely recognition of critical illness is associated with improved outcomes, but is dependent on accurate triage, which is affected by system factors such as workload and staffing. We sought to first study the effect of delayed recognition on patient outcomes after controlling for system factors and then to identify potential predictors of delayed recognition.
Methods: We conducted a retrospective cohort study of Emergency Department (ED) patients admitted to the Intensive Care Unit (ICU) directly from the ED or within 48 hours of ED departure. Cohort characteristics were obtained through electronic and standardized chart abstraction. Operational metrics to estimate ED workload and volume using census data were matched to patients' ED stays. Delayed recognition of critical illness was defined as an absence of an ICU consult in the ED or declination of ICU admission by the ICU team. We employed entropy-balanced multivariate models to examine the association between delayed recognition and development of persistent organ dysfunction and/or death by hospitalization day 28 (POD+D), and multivariable regression modeling to identify factors associated with delayed recognition.
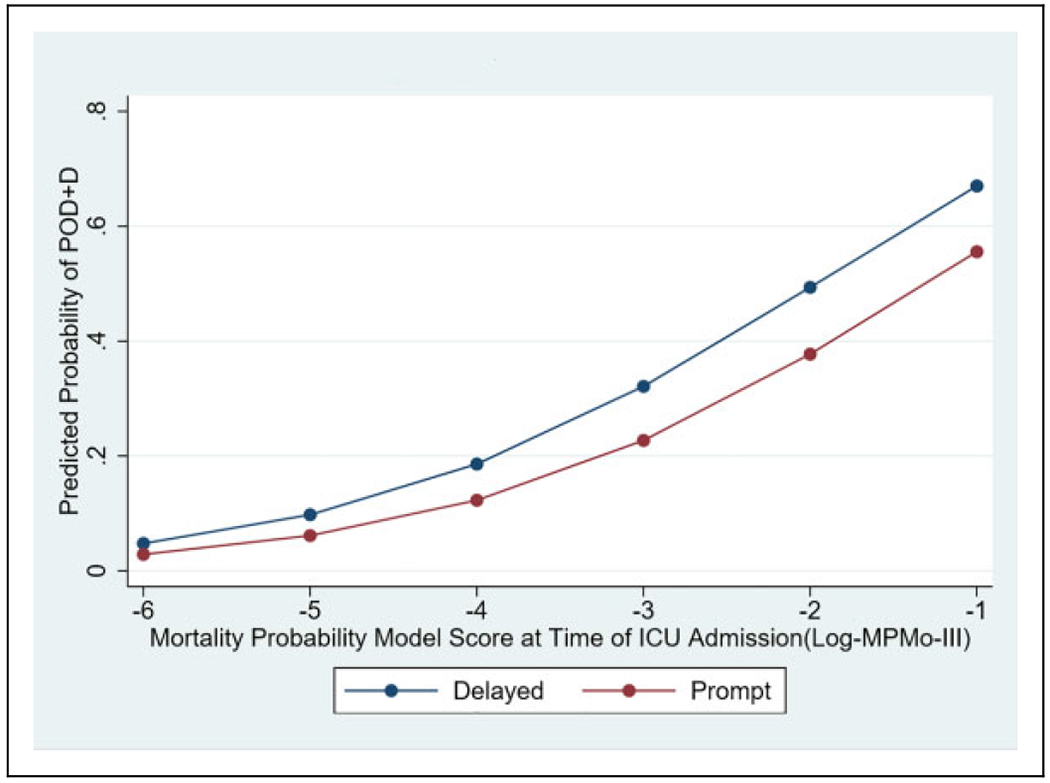
Results: Increased POD+D was seen for those with delayed recognition (OR 1.82, 95% CI 1.13-2.92). When the delayed recognition was by the ICU team, the patient was 2.61 times more likely to experience POD+D compared to those for whom an ICU consult was requested and were accepted for admission. Lower initial severity of illness score (OR 0.26, 95% CI 0.12-0.53) was predictive of delayed recognition. The odds for delayed recognition decreased when ED workload is higher (OR 0.45, 95% CI 0.23-0.89) compared to times with lower ED workload.
Conclusions: Increased POD+D is associated with delayed recognition. Patient and system factors such as severity of illness and ED workload influence the odds of delayed recognition of critical illness and need further exploration.
Keywords: ED boarding; ED crowding; critically ill; emergency department (ED); time-to-treatment.
Figures
References
-
- Gopalan PD, Pershad S. Decision-making in ICU—a systematic review of factors considered important by ICU clinician decision makers with regard to ICU triage decisions. J Crit Care. 2019;50: 99–110. - PubMed
-
- Chalfin DB, Trzeciak S, Likourezos A, Baumann BM, Dellinger RP; Delay-ED study group. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477–1483. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
