

Clinical management of cerebral small vessel disease: a call for a holistic approach
- PMID: 33118960
- PMCID: PMC7817338
- DOI: 10.1097/CM9.0000000000001177
Clinical management of cerebral small vessel disease: a call for a holistic approach
Abstract
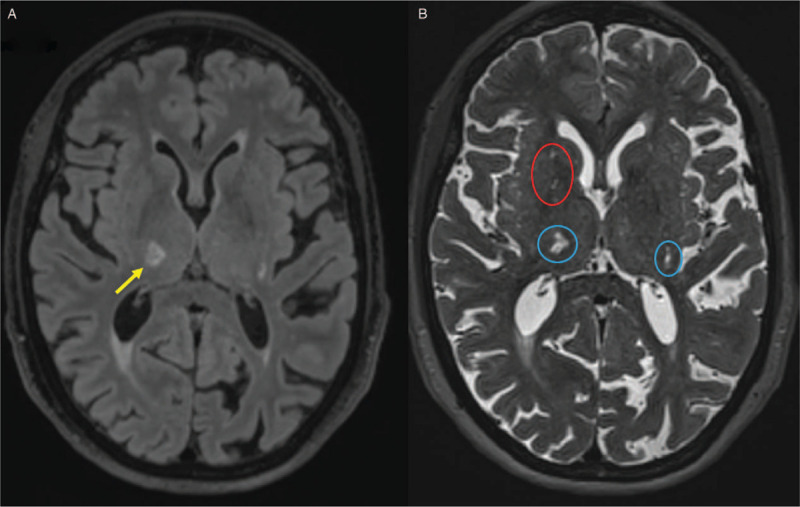
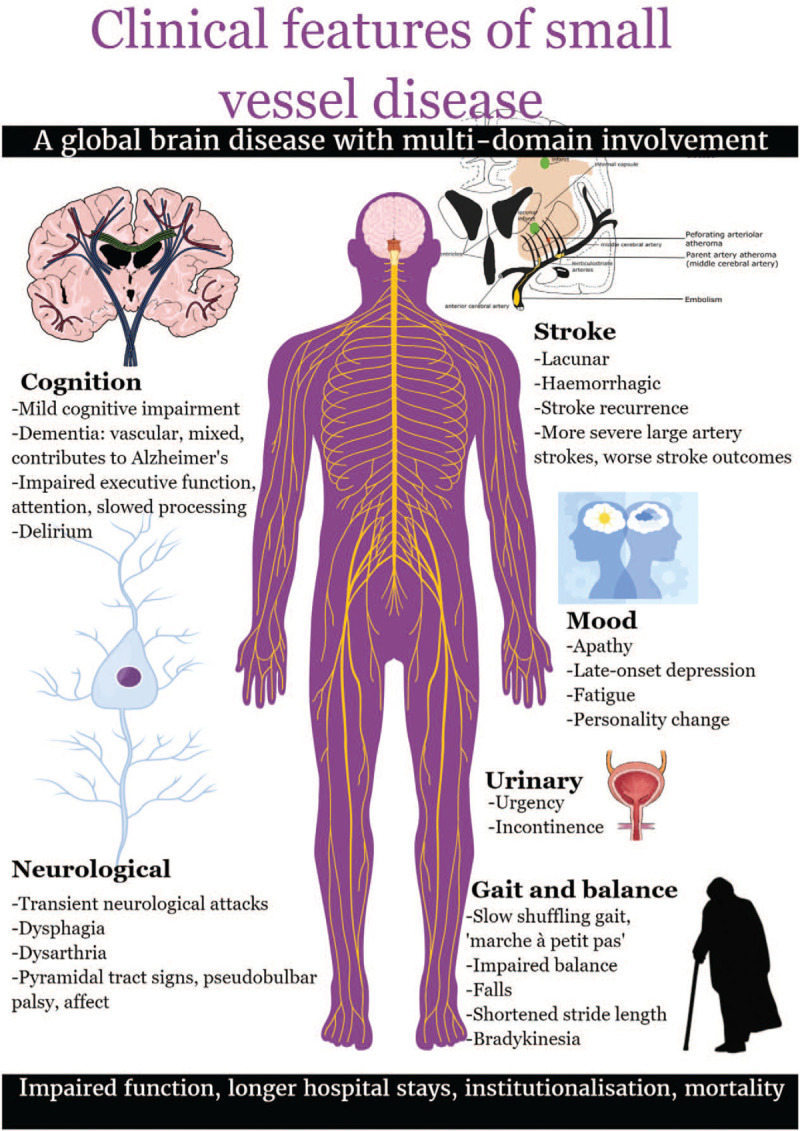
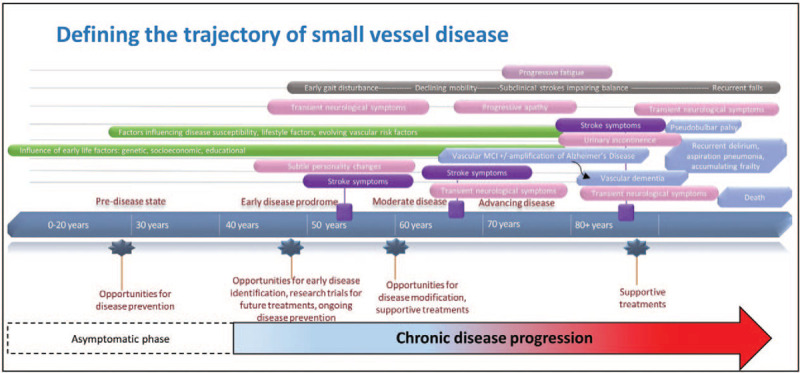
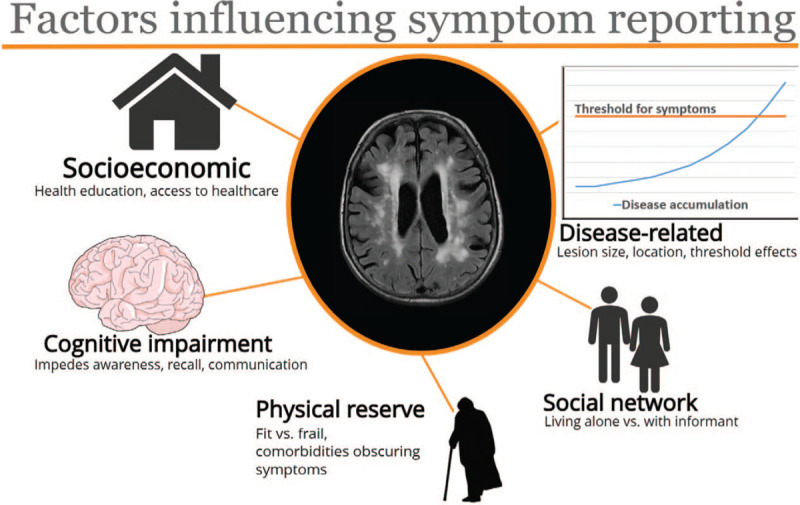
Cerebral small vessel disease (SVD) is a common global brain disease that causes cognitive impairment, ischemic or hemorrhagic stroke, problems with mobility, and neuropsychiatric symptoms. The brain damage, seen as focal white and deep grey matter lesions on brain magnetic resonance imaging (MRI) or computed tomography (CT), typically accumulates "covertly" and may reach an advanced state before being detected incidentally on brain scanning or causing symptoms. Patients have typically presented to different clinical services or been recruited into research focused on one clinical manifestation, perhaps explaining a lack of awareness, until recently, of the full range and complexity of SVD.In this review, we discuss the varied clinical presentations, established and emerging risk factors, relationship to SVD features on MRI or CT, and the current state of knowledge on the effectiveness of a wide range of pharmacological and lifestyle interventions. The core message is that effective assessment and clinical management of patients with SVD, as well as future advances in diagnosis, care, and treatment, will require a more "joined-up"' approach. This approach should integrate clinical expertise in stroke neurology, cognitive, and physical dysfunctions. It requires more clinical trials in order to improve pharmacological interventions, lifestyle and dietary modifications. A deeper understanding of the pathophysiology of SVD is required to steer the identification of novel interventions. An essential prerequisite to accelerating clinical trials is to improve the consistency, and standardization of clinical, cognitive and neuroimaging endpoints.
Copyright © 2020 The Chinese Medical Association, produced by Wolters Kluwer, Inc. under the CC-BY-NC-ND license.
Conflict of interest statement
Conflicts of interest: The authors declare academic grants for research as listed above; JMW chairs the ESOC 2021 Planning Group, and participates in two ESO Guidelines; CA, JPA and UC have no conflicts to disclose. PMB has received honoraria as Chief Investigator or Steering Committee Chair of trials (DiaMedica, Phagenesis) and attending Advisory Boards (Moleac, Nestle, Sanofi).
Figures
References
-
- Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol 2010; 9:689–701. doi: 10.1016/S1474-4422(10)70104-6. - PubMed
-
- Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol 2019; 18:684–696. doi: 10.1016/S1474-4422(19)30079-1. - PubMed
-
- Bos D, Wolters FJ, Darweesh SKL, Vernooij MW, de Wolf F, Ikram MA, et al. Cerebral small vessel disease and the risk of dementia: A systematic review and meta-analysis of population-based evidence. Alzheimers Dement 2018; 14:1482–1492. doi: 10.1016/j.jalz.2018.04.007. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
