

Multisystem Immune-Related Adverse Events Associated With Immune Checkpoint Inhibitors for Treatment of Non-Small Cell Lung Cancer
- PMID: 33119034
- PMCID: PMC7596677
- DOI: 10.1001/jamaoncol.2020.5012
Multisystem Immune-Related Adverse Events Associated With Immune Checkpoint Inhibitors for Treatment of Non-Small Cell Lung Cancer
Abstract
Importance: The spectrum of individual immune-related adverse events (irAEs) from anti-programmed cell death 1 (PD-1) and programmed cell death ligand 1 (PD-L1) immune checkpoint inhibitors (ICIs) has been reported widely, and their development is associated with improved patient survival across tumor types. The spectrum and impact on survival for patients with non-small cell lung cancer (NSCLC) who develop multisystem irAEs from ICIs, has not been described.
Objective: To characterize multisystem irAEs, their association with survival, and risk factors for multisystem irAE development.
Design, setting, and participants: This retrospective cohort study carried out in 5 academic institutions worldwide included 623 patients with stage III/IV NSCLC, treated with anti-PD-(L)1 ICIs alone or in combination with another anticancer agent between January 2007 and January 2019.
Exposures: Anti-PD-(L)1 monotherapy or combinations.
Main outcomes and measures: Multisystem irAEs were characterized by combinations of individual irAEs or organ system involved, separated by ICI-monotherapy or combinations. Median progression-free (PFS) and overall survival (OS) were estimated using the Kaplan-Meier method. Differences in PFS and OS between irAE groups were assessed by multivariable models. Risk for multisystem irAE was estimated as odds ratios by multivariable logistic regression.
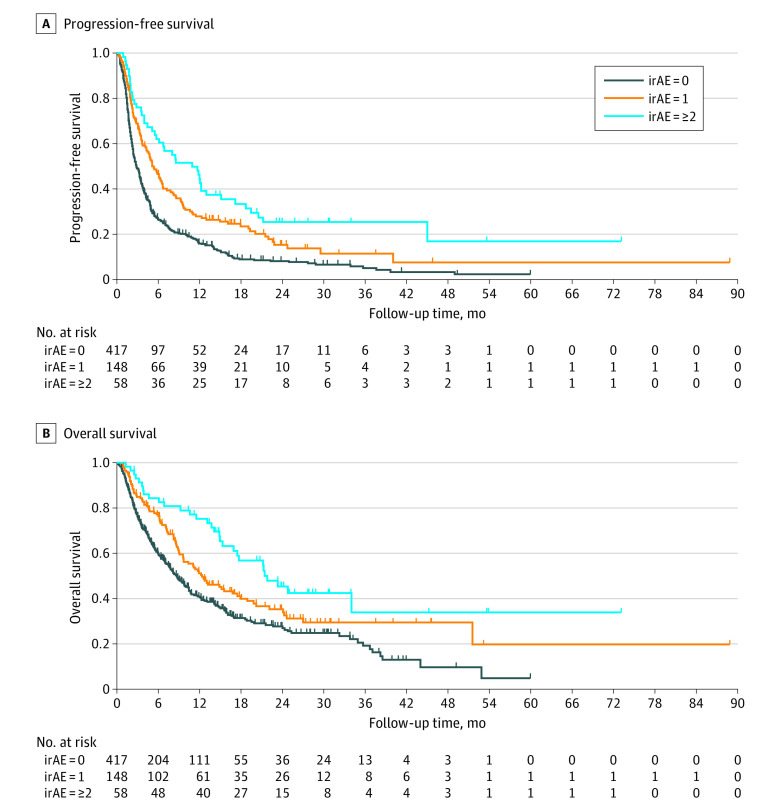
Results: The 623 patients included in the study were mostly men (60%, n = 375) and White (77%, n = 480). The median (range) age was 66 (58-73) years, and 148 patients (24%) developed a single irAE, whereas 58 (9.3%) developed multisystem irAEs. The most common multisystem irAE patterns in patients receiving anti-PD-(L)1 monotherapy were pneumonitis thyroiditis (n = 7, 14%), hepatitis thyroiditis (n = 5, 10%), dermatitis pneumonitis (n = 5, 10%), and dermatitis thyroiditis (n = 4, 8%). Favorable Eastern Cooperative Oncology Group (ECOG) performance status (PS) (ECOG PS = 0/1 vs 2; adjusted odds ratio [aOR], 0.27; 95% CI, 0.08-0.94; P = .04) and longer ICI duration (aOR, 1.02; 95% CI, 1.01-1.03; P < .001) were independent risk factors for development of multisystem irAEs. Patients with 1 irAE and multisystem irAEs demonstrated incrementally improved OS (adjusted hazard ratios [aHRs], 0.86; 95% CI, 0.66-1.12; P = .26; and aHR, 0.57; 95% CI, 0.38-0.85; P = . 005, respectively) and PFS (aHR, 0.68; 95% CI, 0.55-0.85; P = .001; and aHR, 0.39; 95% CI, 0.28-0.55; P < .001, respectively) vs patients with no irAEs, in multivariable models adjusting for ICI duration.
Conclusions and relevance: In this multicenter cohort study, development of multisystem irAEs was associated with improved survival in patients with advanced NSCLC treated with ICIs.
Conflict of interest statement
Figures
Comment in
-
Immune-Related Adverse Events and Efficacy-The More It Hurts, the Better It Works?JAMA Oncol. 2021 Jun 1;7(6):944-945. doi: 10.1001/jamaoncol.2021.0729. JAMA Oncol. 2021. PMID: 33914011 No abstract available.
-
Immune-Related Adverse Events and Efficacy-The More It Hurts, the Better It Works?-Reply.JAMA Oncol. 2021 Jun 1;7(6):945. doi: 10.1001/jamaoncol.2021.0732. JAMA Oncol. 2021. PMID: 33914013 No abstract available.
References
-
- Fehrenbacher L, von Pawel J, Park K, et al. Updated efficacy analysis including secondary population results for OAK: a randomized phase III study of atezolizumab versus docetaxel in patients with previously treated advanced non-small cell lung cancer. J Thorac Oncol. 2018;13(8):1156-1170. doi: 10.1016/j.jtho.2018.04.039 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
