

Effectiveness of vergence/accommodative therapy for accommodative dysfunction in children with convergence insufficiency
- PMID: 33119180
- PMCID: PMC10545079
- DOI: 10.1111/opo.12747
Effectiveness of vergence/accommodative therapy for accommodative dysfunction in children with convergence insufficiency
Erratum in
-
Effectiveness of vergence/accommodative therapy for accommodative dysfunction in children with convergence insufficiency.Ophthalmic Physiol Opt. 2023 Jan;43(1):170-172. doi: 10.1111/opo.13064. Epub 2022 Oct 22. Ophthalmic Physiol Opt. 2023. PMID: 36271749 Free PMC article. No abstract available.
Abstract
Purpose: To determine the effectiveness of office-based vergence/accommodative therapy for improving accommodative amplitude and accommodative facility in children with symptomatic convergence insufficiency and accommodative dysfunction.
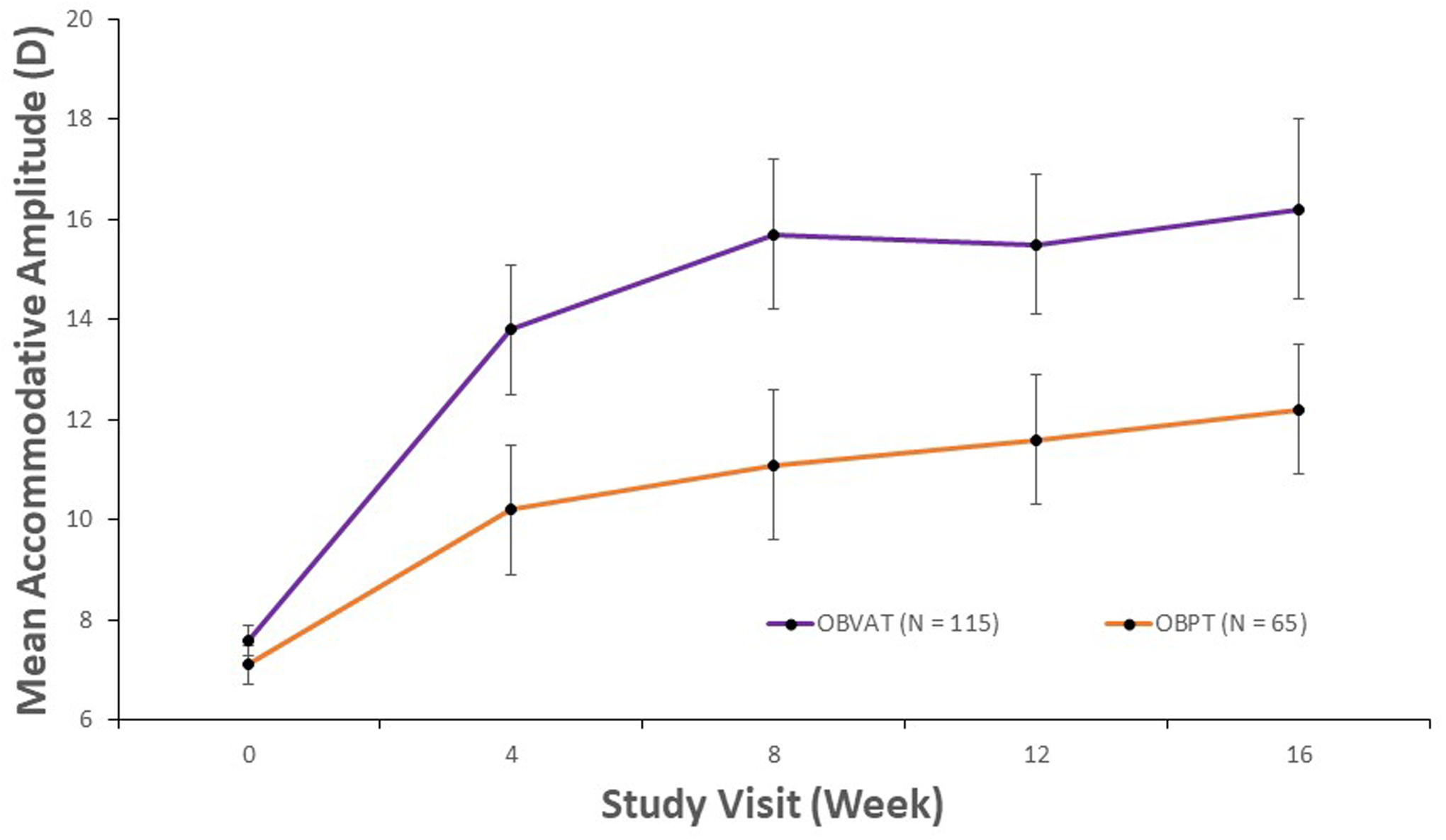
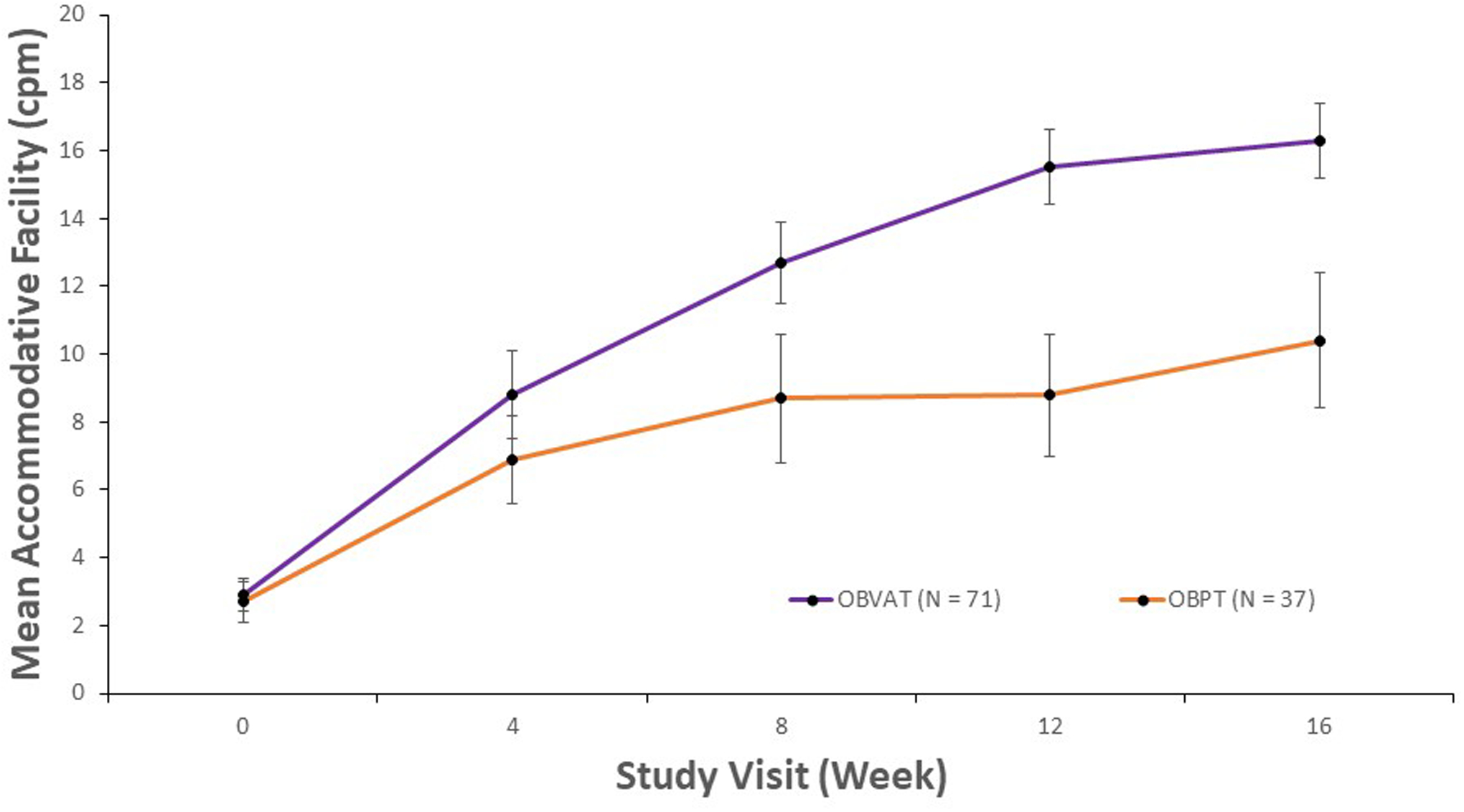
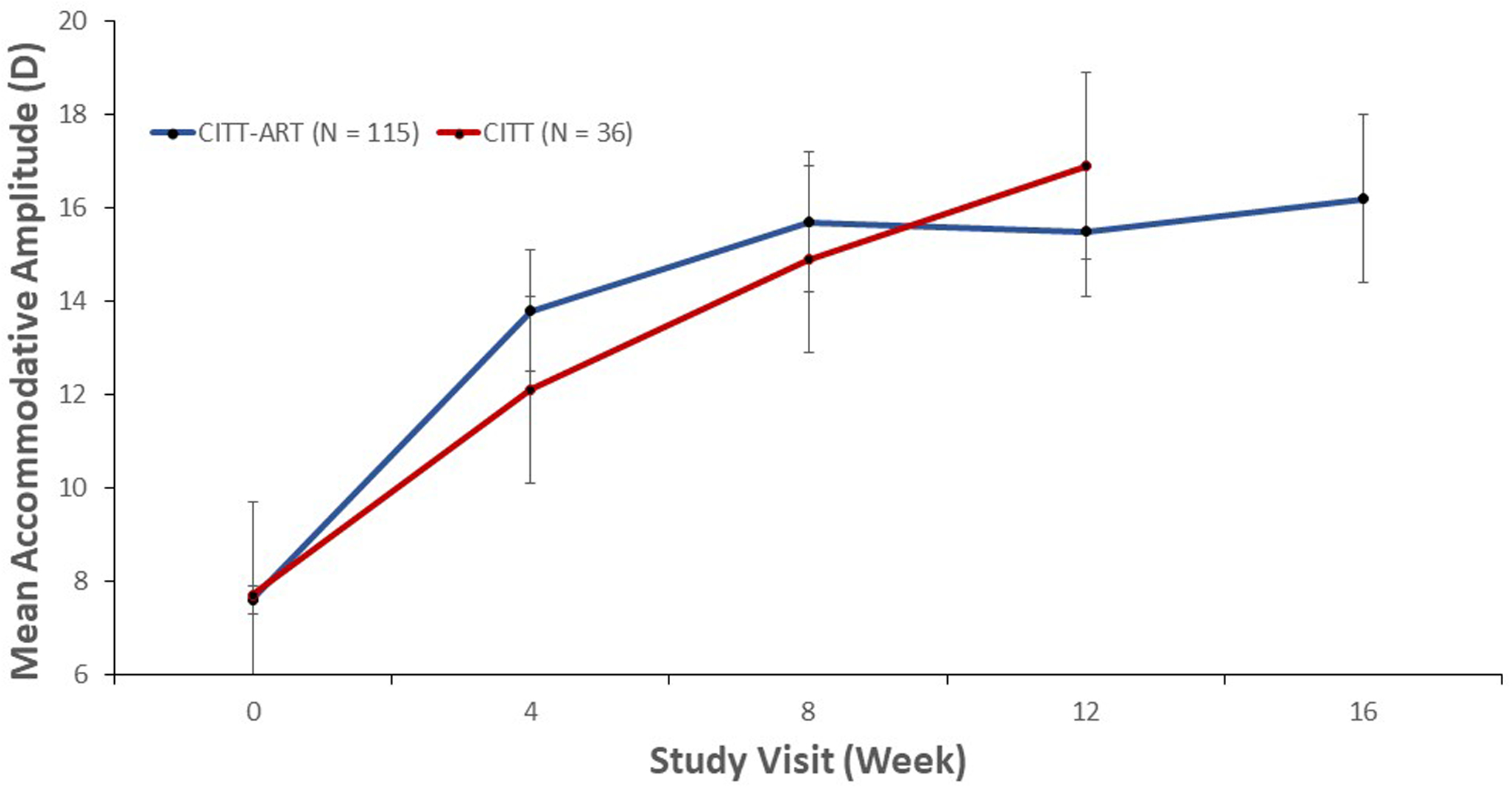
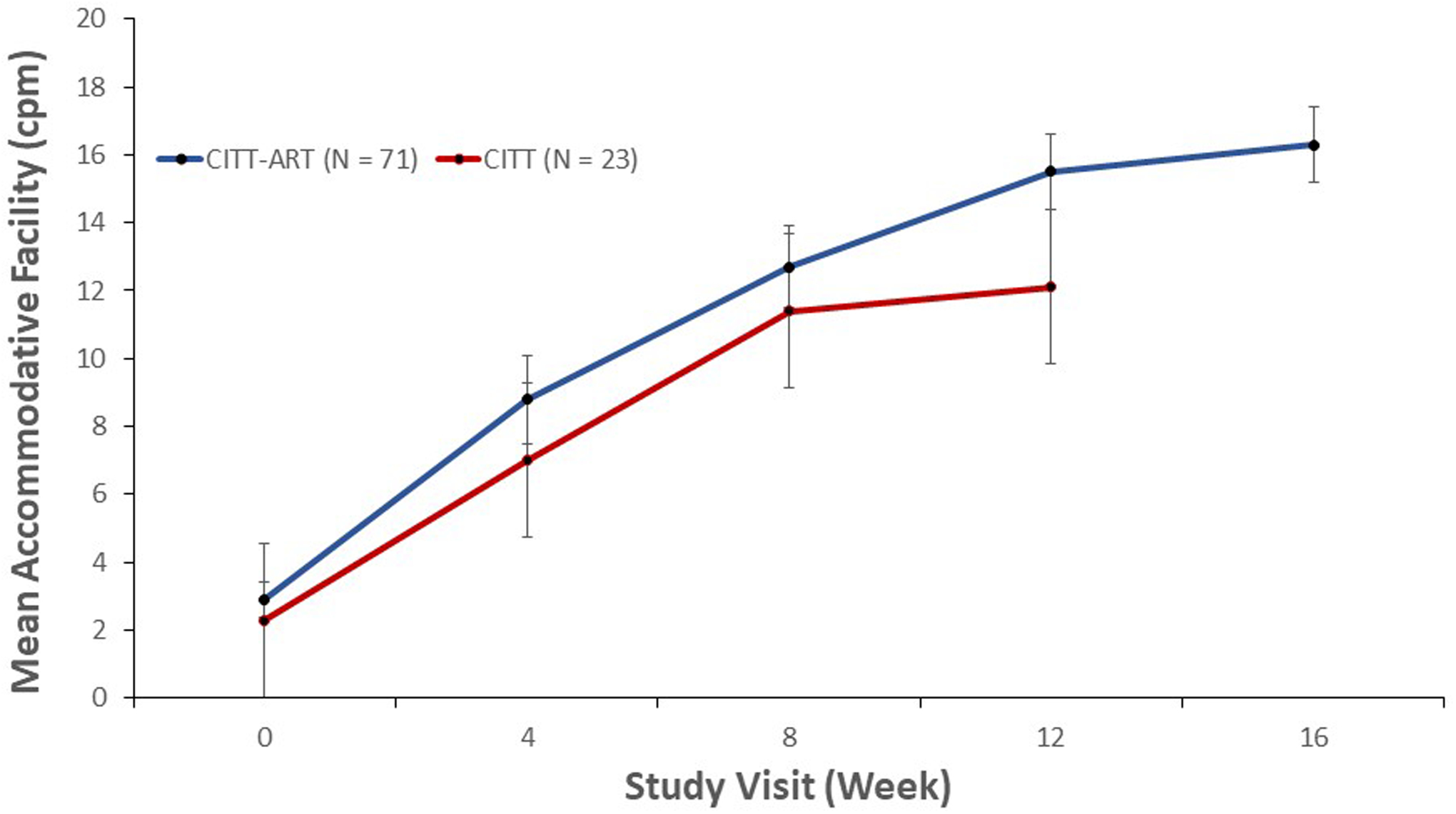
Methods: We report changes in accommodative function following therapy among participants in the Convergence Insufficiency Treatment Trial - Attention and Reading Trial with decreased accommodative amplitude (115 participants in vergence/accommodative therapy; 65 in placebo therapy) or decreased accommodative facility (71 participants in vergence/accommodative therapy; 37 in placebo therapy) at baseline. The primary analysis compared mean change in amplitude and facility between the vergence/accommodative and placebo therapy groups using analyses of variance models after 4, 8, 12 and 16 weeks of treatment. The proportions of participants with normal amplitude and facility at each time point were calculated. The average rate of change in amplitude and facility from baseline to week 4, and from weeks 4 to 16, were determined in the vergence/accommodative therapy group.
Results: From baseline to 16 weeks, the mean improvement in amplitude was 8.6 dioptres (D) and 5.2 D in the vergence/accommodative and placebo therapy groups, respectively (mean difference = 3.5 D, 95% confidence interval (CI): 1.5 to 5.5 D; p = 0.01). The mean improvement in facility was 13.5 cycles per minute (cpm) and 7.6 cpm in the vergence/accommodative and placebo therapy groups, respectively (mean difference = 5.8 cpm, 95% CI: 3.8 to 7.9 cpm; p < 0.0001). Significantly greater proportions of participants treated with vergence/accommodative therapy achieved a normal amplitude (69% vs. 32%, difference = 37%, 95% CI: 22 to 51%; p < 0.0001) and facility (85% vs. 49%, difference = 36%, 95% CI: 18 to 55%; p < 0.0001) than those who received placebo therapy. In the vergence/accommodative therapy group, amplitude increased at an average rate of 1.5 D per week during the first 4 weeks (p < 0.0001), then slowed to 0.2 D per week (p = 0.002) from weeks 4 to 16. Similarly, facility increased at an average rate of 1.5 cpm per week during the first 4 weeks (p < 0.0001), then slowed to 0.6 cpm per week from weeks 4 to 16 (p < 0.0001).
Conclusion: Office-based vergence/accommodative therapy is effective for improving accommodative function in children with symptomatic convergence insufficiency and coexisting accommodative dysfunction.
Keywords: accommodative amplitude; accommodative dysfunction; accommodative facility; convergence insufficiency; vergence/accommodative therapy.
© 2020 The Authors Ophthalmic & Physiological Optics © 2020 The College of Optometrists.
Conflict of interest statement
Figures
References
-
- Hussaindeen JR, Rakshit A, Singh NK, et al. Prevalence of non-strabismic anomalies of binocular vision in Tamil Nadu: report 2 of BAND study. Clin Exp Optom 2017;100:642–8. - PubMed
-
- Wajuihian SO, Hansraj R. Accommodative Anomalies in a Sample of Black High School Students in South Africa. Ophthalmic Epidemiol 2016;23:316–23. - PubMed
-
- Daum K. Accommodative dysfunction. Doc Ophthalmol 1983;61:177–83. - PubMed
-
- Hennessey D, Iosue R, Rouse M. Relation of symptoms to accommodative infacility of school-aged children. Am J Optom Physiol Opt 1984:177–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
