

Altered airway mechanics in the context of obesity and asthma
- PMID: 33119471
- PMCID: PMC7944930
- DOI: 10.1152/japplphysiol.00666.2020
Altered airway mechanics in the context of obesity and asthma
Abstract
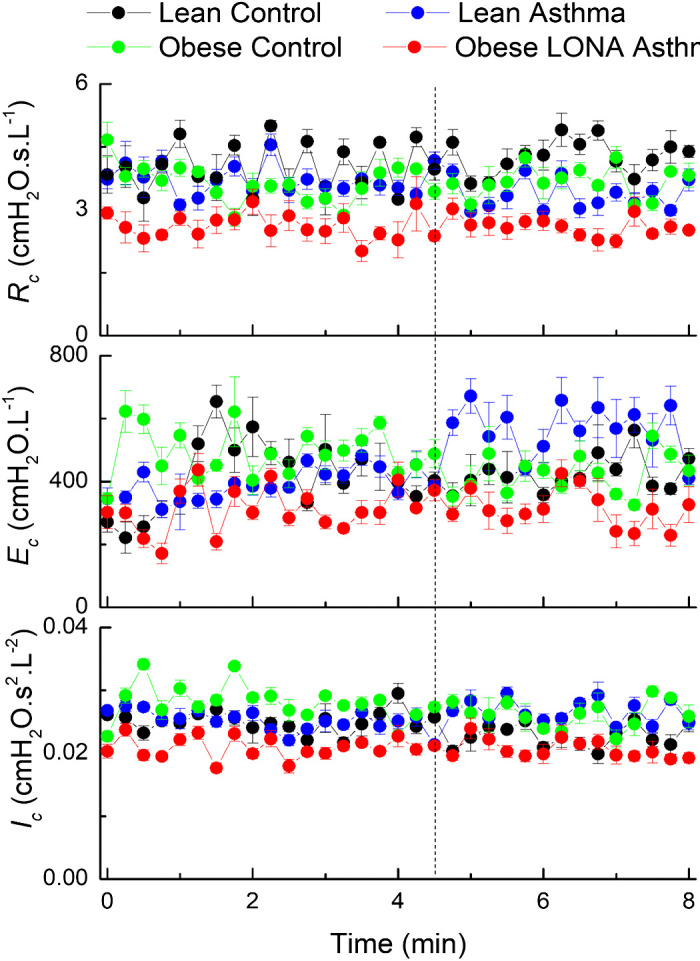
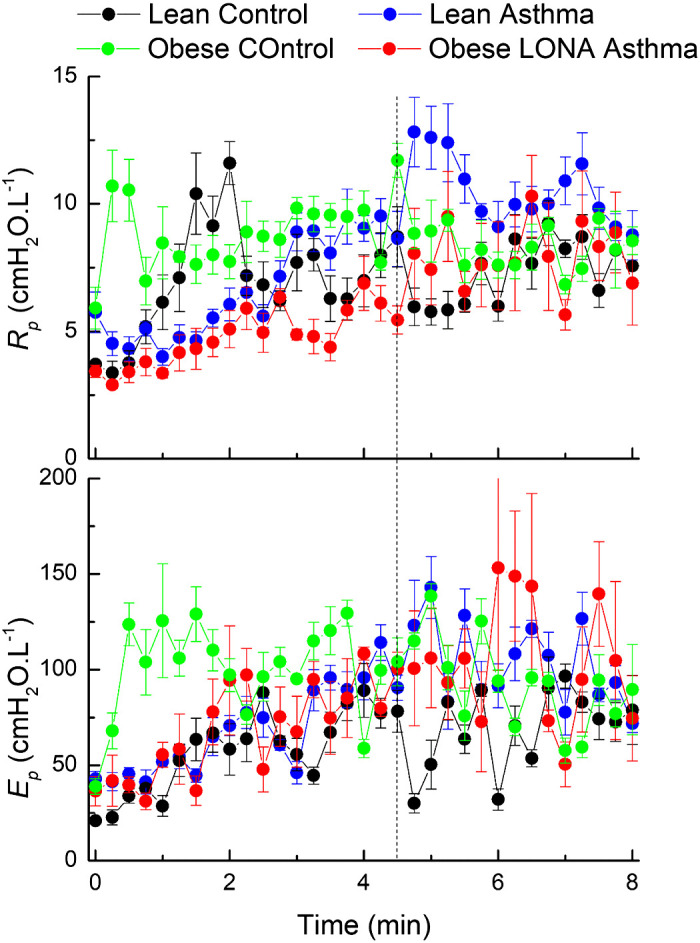
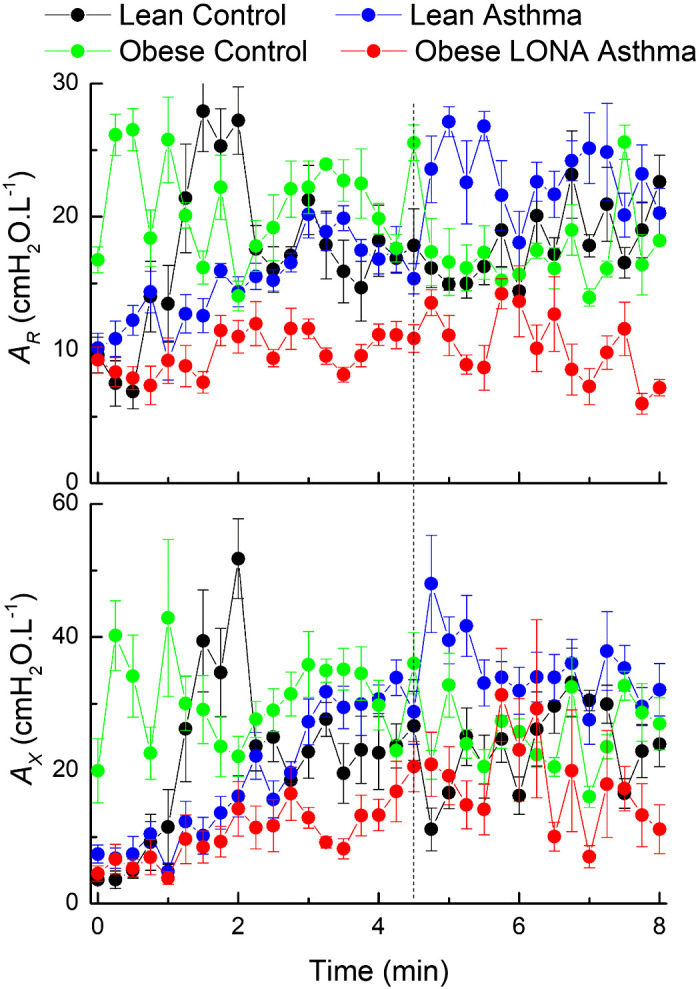
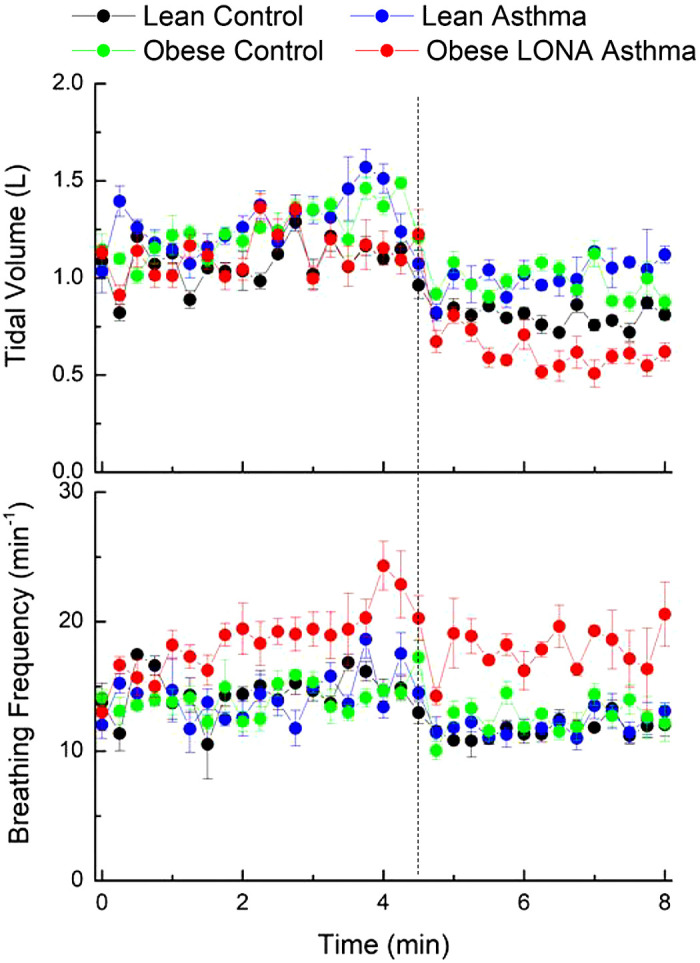
The obesity epidemic is causing a rise in asthma incidence due to the appearance of an obesity-specific late-onset nonallergic (LONA) phenotype. We investigated why only a subset of obese participants develop LONA asthma by determining how obesity, both alone and in combination with LONA asthma, affects the volume dependence of respiratory system impedance. We also determined how obesity and asthma affect impedance during and following challenge with the PC20 dose of methacholine. We found during passive exhalation that all obese participants, in contrast to lean controls and lean asthmatics, experienced similarly profound elevations in lung elastance as they approached functional residual capacity. We also found, however, that the LONA asthmatics had a greater negative dependence of airway resistance on lung volume over the middle of the volume range compared with the other groups. Methacholine challenge with the PC20 dose led to comparable changes in respiratory system impedance in the four study groups, but the doses themselves were substantially lower in both obese and lean asthmatic participants compared with obese and lean controls. Also, the obese LONA asthmatics had higher breathing frequencies and lower tidal volumes postchallenge compared with the other participants. Taken together, these results suggest that all obese individuals experience substantial lung collapse as they approach functional residual capacity, presumably due to the weight of the chest wall. It remains unclear why obese LONA asthmatics are hyperresponsive to methacholine while obese nonasthmatic individuals are not.NEW & NOTEWORTHY Why only a subset of severely obese subjects develop late-onset nonallergic (LONA) asthma remains unknown, although it is widely assumed that compression of the lungs by the chest wall is somehow involved. We show that lung compression is common to obese individuals both without asthma and with LONA asthma but that those with LONA asthma may have increased airway wall compliance and possibly also a reduced ability to recruit collapsed lung.
Keywords: airway resistance; airway wall compliance; mathematical model; respiratory system impedance.
Figures
Comment in
-
Recovery after histamine challenge test: effect of gender and body mass index.J Appl Physiol (1985). 2023 Aug 1;135(2):300-301. doi: 10.1152/japplphysiol.00319.2023. J Appl Physiol (1985). 2023. PMID: 37470780 No abstract available.
References
-
- Holguin F, Bleecker ER, Busse WW, Calhoun WJ, Castro M, Erzurum SC, Fitzpatrick AM, Gaston B, Israel E, Jarjour NN, Moore WC, Peters SP, Yonas M, Teague WG, Wenzel SE. Obesity and asthma: an association modified by age of asthma onset. J Allergy Clin Immunol 127: 1486–1493, 2011. doi:10.1016/j.jaci.2011.03.036. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases