

Multicenter, Randomized, Phase III Trial of Neoadjuvant Chemoradiation With Capecitabine and Irinotecan Guided by UGT1A1 Status in Patients With Locally Advanced Rectal Cancer
- PMID: 33119477
- PMCID: PMC7768334
- DOI: 10.1200/JCO.20.01932
Multicenter, Randomized, Phase III Trial of Neoadjuvant Chemoradiation With Capecitabine and Irinotecan Guided by UGT1A1 Status in Patients With Locally Advanced Rectal Cancer
Abstract
Purpose: Differentiating the irinotecan dose on the basis of the uridine diphosphate glucuronosyltransferase 1A1 (UGT1A1) genotype improves the pathologic complete response (pCR) rate. In this study, we further investigated preoperative irinotecan combined with capecitabine-based chemoradiotherapy for locally advanced rectal cancer.
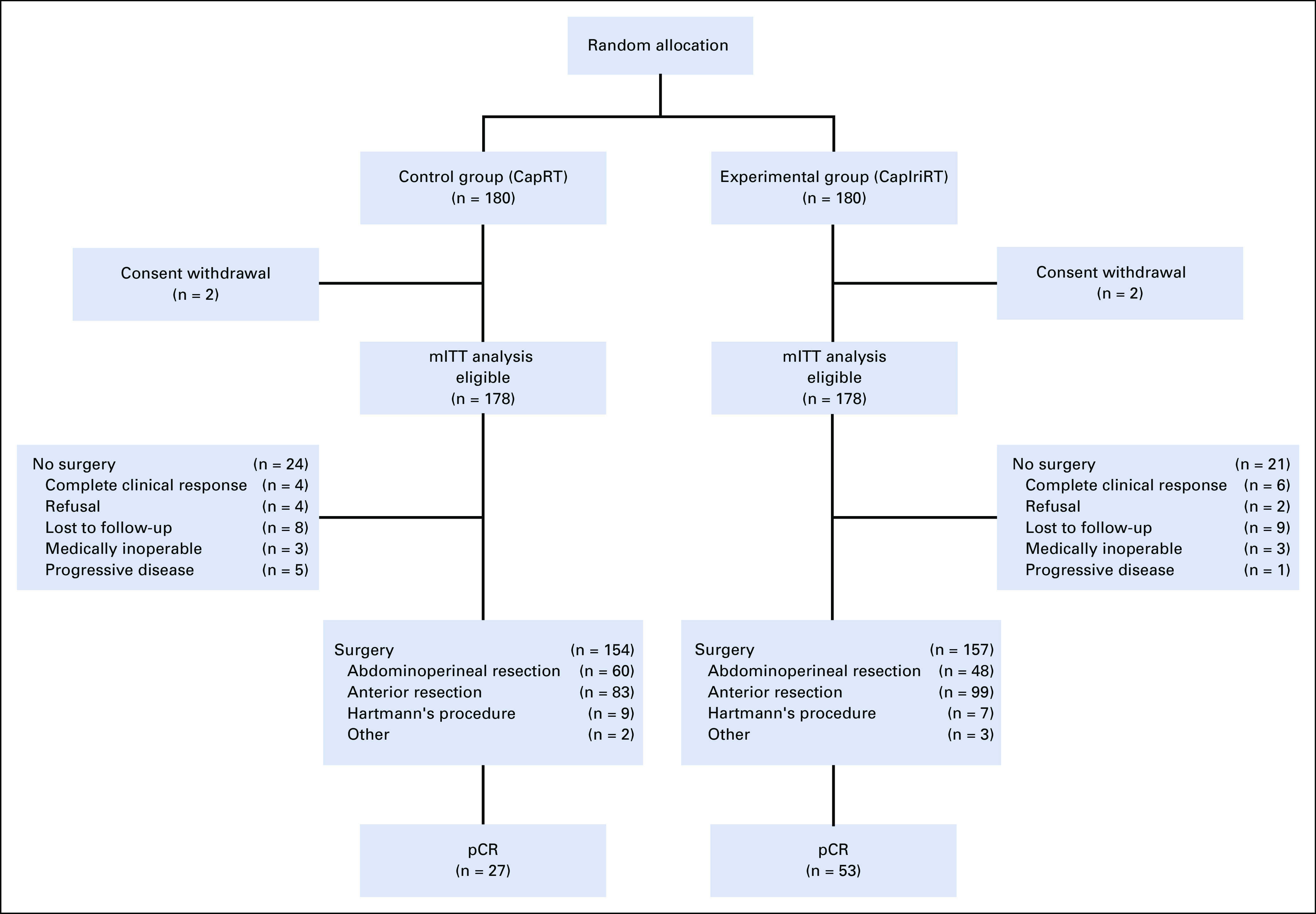
Patients and methods: We conducted this randomized, open-label, multicenter, phase III trial in China. Eligible patients with clinical T3-4 and/or N+ rectal adenocarcinoma, UGT1A1 genotype *1*1 or *1*28 were randomly allocated to the control group: pelvic radiation of 50 Gy/25 fractions with concurrent capecitabine, followed by oxaliplatin and capecitabine; or the experimental group: radiation with capecitabine combined with weekly irinotecan 80 mg/m2 for patients with UGT1A1*1*1 or 65 mg/m2 for patients with UGT1A1*1*28, followed by irinotecan and capecitabine. The primary end point was pCR. This trial was registered with ClinicalTrials.gov (ClinicalTrials.gov identifier: NCT02605265).
Results: Of the 360 patients initially enrolled, 356 were evaluated as the modified intention-to-treat population (n = 178 in both groups). Surgery was performed in 87% and 88% of patients in the control and experimental groups, respectively. The pCR rates were 15% (n = 27 of 178) and 30% (n = 53 of 178) in the control and experimental groups (risk ratio, 1.96; 95% CI, 1.30 to 2.97; P = .001). Four and 6 patients achieved complete clinical response in the control and experimental groups, respectively. Grade 3-4 toxicities were recorded in 11 (6%) and 68 (38%) patients in the control and experimental groups, respectively (P < .001). The commonest grade 3-4 toxicities were leukopenia, neutropenia, and diarrhea. The overall surgical complication rate was not significantly different between the two groups (11% v 15%; P < .001).
Conclusion: Adding irinotecan guided by UGT1A1 genotype to capecitabine-based neoadjuvant chemoradiotherapy significantly increased complete tumor response in Chinese patients.
Figures
References
-
- Sauer R Becker H Hohenberger W, et al. : Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 351:1731-1740, 2004 - PubMed
-
- Sauer R Liersch T Merkel S, et al. : Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: Results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol 30:1926-1933, 2012 - PubMed
-
- Hartley A Ho KF McConkey C, et al. : Pathological complete response following pre-operative chemoradiotherapy in rectal cancer: Analysis of phase II/III trials. Br J Radiol 78:934-938, 2005 - PubMed
-
- Deng Y Chi P Lan P, et al. : Modified FOLFOX6 with or without radiation versus fluorouracil and leucovorin with radiation in neoadjuvant treatment of locally advanced rectal cancer: Initial results of the Chinese FOWARC multicenter, open-label, randomized three-arm phase III trial. J Clin Oncol 34:3300-3307, 2016 - PubMed
-
- Rödel C Graeven U Fietkau R, et al. : Oxaliplatin added to fluorouracil-based preoperative chemoradiotherapy and postoperative chemotherapy of locally advanced rectal cancer (the German CAO/ARO/AIO-04 study): Final results of the multicentre, open-label, randomised, phase 3 trial. Lancet Oncol 16:979-989, 2015 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
