

A comparison between laparoscopy and hysteroscopy approach in treatment of cesarean scar pregnancy
- PMID: 33120815
- PMCID: PMC7581091
- DOI: 10.1097/MD.0000000000022845
A comparison between laparoscopy and hysteroscopy approach in treatment of cesarean scar pregnancy
Abstract
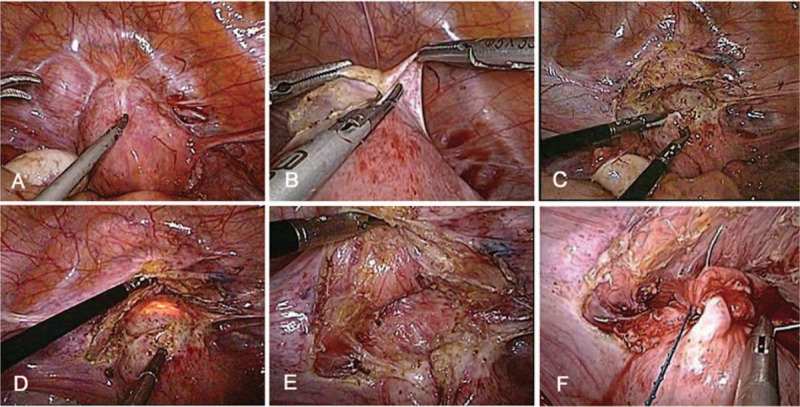
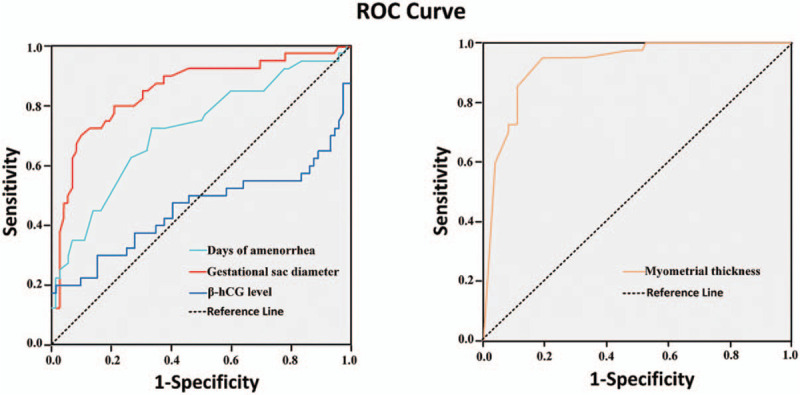
The aim of the study was to compare the efficacy of laparoscopy and hysteroscopy for the treatment of cesarean scar pregnancy (CSP) and analyze the clinical factors associated with successful selection for hysteroscopic or laparoscopic treatment of CSP.We retrospectively studied 112 cases of CSP that were treated by laparoscopy and/or hysteroscopy in our hospital from December 2014 to December 2017. In total, 72 of these patients underwent ultrasound-guided curettage and hysteroscopic resection without uterine scar defect repair. Fourty of these patients underwent laparoscopic resection and repair of the uterine scar defect. We analyzed the different clinical variables between the 2 groups and identified the clinical factors which could predict the need for the laparoscopic repair of uterine scar defect. Results showed that laparoscopy and hysteroscopy were safe ways to treat CSP, and no patient underwent hysterectomy. The β-hCG level in both of the 2 groups decreased to normal 4 to 8 weeks after surgery. There were significant differences between the hysteroscopy group and laparoscopy uterine scar repair group in terms of days of amenorrhea, gestational sac diameter, myometrial thickness, operation time, intraoperative blood loss, and hospitalization duration (P < .05). Logistic regression analysis showed that the days of amenorrhea, gestational sac diameter and myometrial thickness were independent risk factors for CSP treated by minimally invasive surgery, which were also shown by ROC curve analysis to be predictors of the need for the repair of the uterine scar defect, with optimal cutoffs of 52.50 days, 3.25 cm, and 2.05 mm, respectively; and the areas under their corresponding ROC were 0.721, 0.851, and 0.927, respectively.We conclude that laparoscopy and hysteroscopy are safe and efficient minimally invasive procedures for the treatment of CSP. The days of amenorrhea, gestational sac diameter and myometrial thickness may be key factors associated with successful selection for hysteroscopic or laparoscopic treatment of CSP.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
Similar articles
-
Surgical treatment of cesarean scar pregnancy based on the three-category system: a retrospective analysis.BMC Pregnancy Childbirth. 2024 Oct 21;24(1):687. doi: 10.1186/s12884-024-06887-0. BMC Pregnancy Childbirth. 2024. PMID: 39433995 Free PMC article.
-
Hysteroscopic removal, with or without laparoscopic assistance, of first-trimester cesarean scar pregnancy.Fertil Steril. 2022 Mar;117(3):643-645. doi: 10.1016/j.fertnstert.2021.11.027. Fertil Steril. 2022. PMID: 35219475
-
Clinical Efficacy of Combined Hysteroscopic and Laparoscopic Surgery and Reversible Ligation of the Uterine Artery for Excision and Repair of Uterine Scar in Patients with Type II and III Cesarean Scar Pregnancy.Med Sci Monit. 2020 Jun 29;26:e924076. doi: 10.12659/MSM.924076. Med Sci Monit. 2020. PMID: 32595205 Free PMC article.
-
Laparoscopic treatment of cesarean scar pregnancy: A scoping review.Eur J Obstet Gynecol Reprod Biol. 2025 Apr;307:154-163. doi: 10.1016/j.ejogrb.2025.02.006. Epub 2025 Feb 6. Eur J Obstet Gynecol Reprod Biol. 2025. PMID: 39929117
-
Should Cesarean Scar Defect Be Treated Laparoscopically? A Case Report and Review of the Literature.J Minim Invasive Gynecol. 2015 Nov-Dec;22(7):1145-52. doi: 10.1016/j.jmig.2015.06.013. Epub 2015 Jun 26. J Minim Invasive Gynecol. 2015. PMID: 26122897 Review.
Cited by
-
Approaches in the Treatment of Cesarean Scar Pregnancy and Risk Factors for Intraoperative Hemorrhage: A Retrospective Study.Front Med (Lausanne). 2021 Jun 24;8:682368. doi: 10.3389/fmed.2021.682368. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34249974 Free PMC article.
-
Conservative Management of Cesarean Scar Pregnancy: A Case Report and Literature Review.Case Rep Obstet Gynecol. 2022 Jun 22;2022:1793943. doi: 10.1155/2022/1793943. eCollection 2022. Case Rep Obstet Gynecol. 2022. PMID: 35783220 Free PMC article.
-
Comparing the clinical efficacy of three surgical methods for cesarean scar pregnancy.BMC Womens Health. 2023 May 17;23(1):271. doi: 10.1186/s12905-023-02415-y. BMC Womens Health. 2023. PMID: 37198658 Free PMC article.
-
Prevalence, Determinants, and Management Options of Scar Site Pregnancy in Women With Previous Cesarean Section: A Study From the Al-Qassim Region.Cureus. 2024 Jul 31;16(7):e65874. doi: 10.7759/cureus.65874. eCollection 2024 Jul. Cureus. 2024. PMID: 39219911 Free PMC article.
-
Comparison of Diagnostic Efficacy among Transvaginal Sonography, Transabdominal Sonography, and 3.0 T Magnetic Resonance Imaging in Early Cesarean Scar Pregnancy.J Healthc Eng. 2022 Jan 25;2022:9714369. doi: 10.1155/2022/9714369. eCollection 2022. J Healthc Eng. 2022. PMID: 35126959 Free PMC article.
References
-
- Ash A, Smith A, Maxwell D. Caesarean scar pregnancy. BJOG 2007;114:253–63. - PubMed
-
- Litwicka K, Greco E. Caesarean scar pregnancy: a review of management options. Curr Opin Obstet Gynecol 2011;23:415–21. - PubMed
-
- Rajakumar C, Agarwal S, Khalil H, et al. Caesarean scar pregnancy. J Obstet Gynaecol Can 2015;37:199. - PubMed
-
- Uysal F, Uysal A, Adam G. Cesarean scar pregnancy: diagnosis, management, and follow-up. J Ultrasound Med 2013;32:1295–300. - PubMed
