

Risk factors and outcomes of myocardial injury after non-cardiac surgery in high-risk patients who underwent radical cystectomy
- PMID: 33120837
- PMCID: PMC7581156
- DOI: 10.1097/MD.0000000000022893
Risk factors and outcomes of myocardial injury after non-cardiac surgery in high-risk patients who underwent radical cystectomy
Abstract
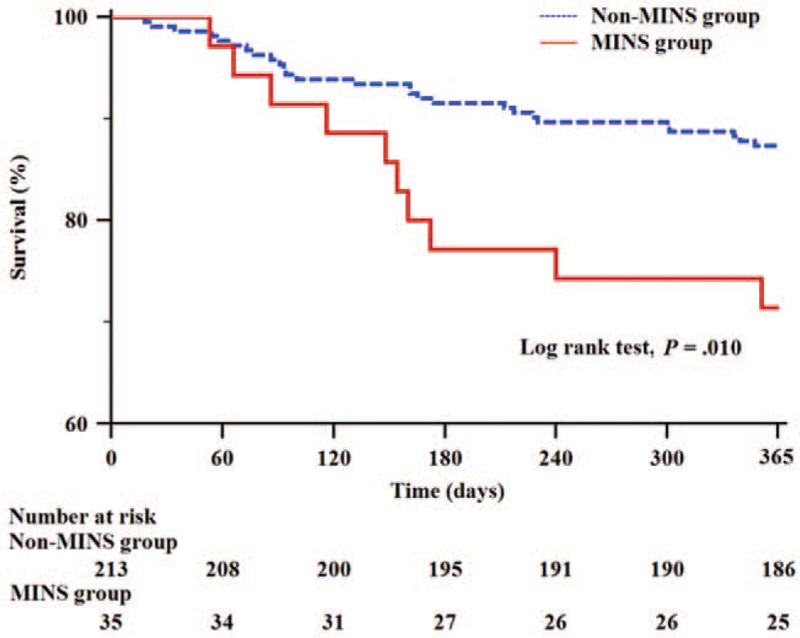
Radical cystectomy is considered the standard treatment for patients with muscle-invasive bladder tumors and has high postoperative complication rates among urological surgeries. High-risk patients, defined as those ≥45 years of age with history of coronary artery disease, stroke, or peripheral artery disease or those ≥65 years of age, can have a higher incidence of cardiac complications. Therefore, we evaluated the incidence, risk factors, and outcomes of myocardial injury after non-cardiac surgery (MINS) in high-risk patients who underwent radical cystectomy.This retrospective observational study analyzed 248 high-risk patients who underwent radical cystectomy. MINS was defined as serum troponin I concentration ≥0.04 mg/L within postoperative 3 days. The risk factors for MINS were evaluated by multivariate logistic regression analysis. Postoperative outcomes were evaluated. The 1-year survival after radical cystectomy was also compared between patients who developed MINS (MINS group) and those who did not (non-MINS group) by Kaplan-Meier analysis.MINS occurred in 35 patients (14.1%). Multivariate logistic regression analysis showed that early diastolic transmitral filling velocity (E)/early diastolic septal mitral annular velocity (E') ratio (odds ratio = 1.102, 95% confidence interval [1.009-1.203], P = .031) and large volume blood transfusion (odds ratio = 2.745, 95% confidence interval [1.131-6.664], P = .026) were significantly associated with MINS in high-risk patients who underwent radical cystectomy. Major adverse cardiac events and 1-year mortality were significantly higher in the MINS group than in the non-MINS group (17.1% vs 6.1%, P = .035; 28.6% vs 12.7%, P = .021, respectively). Kaplan-Meier analysis showed significantly lower 1-year survival in the MINS group than in the non-MINS group (P = .010).MINS occurred in 14.1% of patients. High E/E' ratio and large volume blood transfusion were risk factors for MINS in high-risk patients who underwent radical cystectomy. Postoperative major adverse cardiac events and 1-year mortality were significantly higher in the MINS group than in the non-MINS group. Preoperative evaluation of risk factors for MINS may provide useful information to detect cardiovascular complications after radical cystectomy in high-risk patients.
Conflict of interest statement
The authors have no funding and conflicts of interests to disclose.
Figures

References
-
- Stenzl A, Cowan NC, De Santis M, et al. The updated EAU guidelines on muscle-invasive and metastatic bladder cancer. Eur Urol 2009;55:815–25. - PubMed
-
- Clark PE, Stein JP, Groshen SG, et al. Radical cystectomy in the elderly: comparison of clincal outcomes between younger and older patients. Cancer 2005;104:36–43. - PubMed
-
- Madeb R, Messing EM. Gender, racial and age differences in bladder cancer incidence and mortality. Urol Oncol 2004;22:86–92. - PubMed
-
- Puelacher C, Lurati Buse G, Seeberger D, et al. Perioperative myocardial injury after noncardiac surgery: incidence, mortality, and characterization. Circulation 2018;137:1221–32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
