

Living donor liver transplantation for idiopathic portal hypertension with extrahepatic portal vein stenosis and splenic artery aneurysms: a case report and review of the literature
- PMID: 33121468
- PMCID: PMC7597044
- DOI: 10.1186/s12893-020-00921-6
Living donor liver transplantation for idiopathic portal hypertension with extrahepatic portal vein stenosis and splenic artery aneurysms: a case report and review of the literature
Abstract
Background: Idiopathic portal hypertension (IPH) generally has a good prognosis and rarely results in liver transplantation. Furthermore, there are few reports of living donor liver transplantation (LDLT) for IPH with extrahepatic portal vein stenosis.
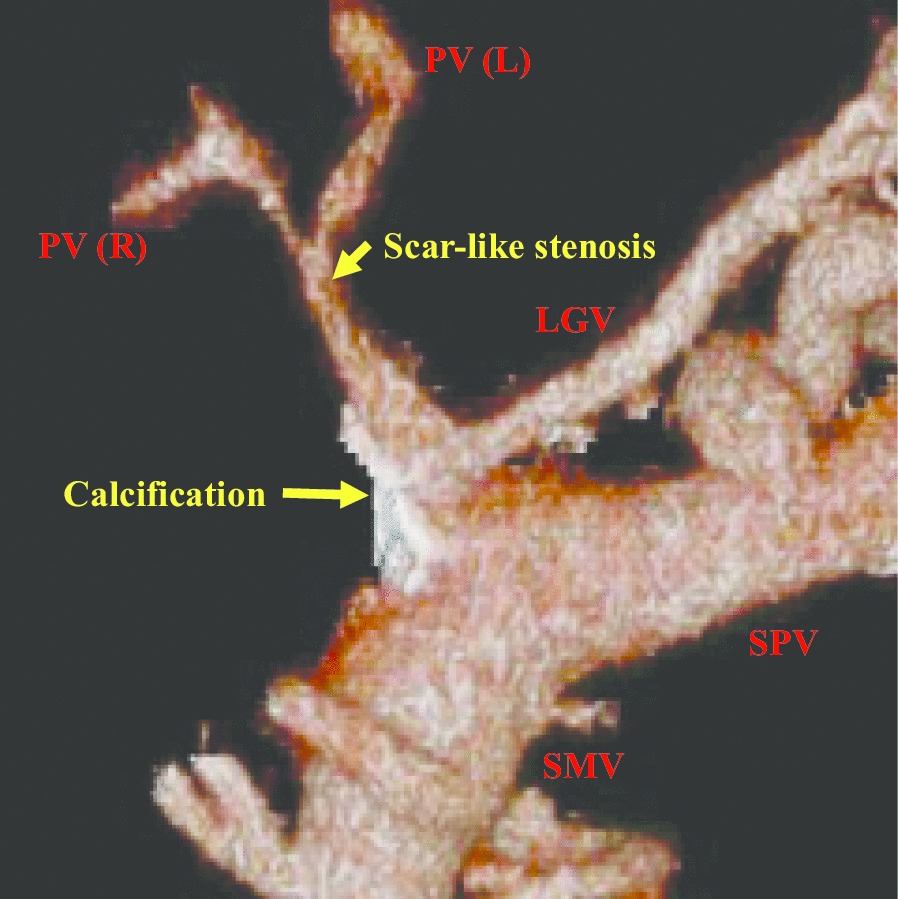
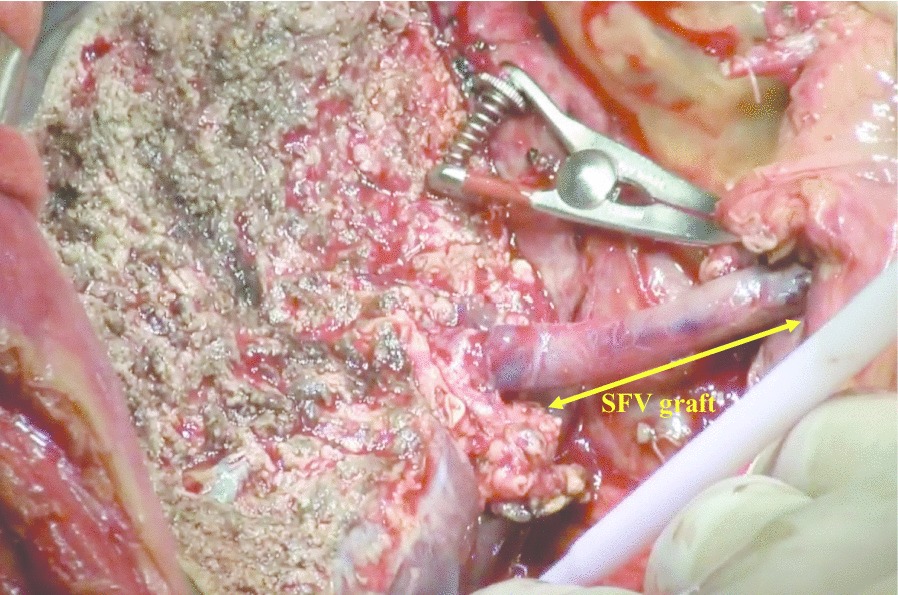
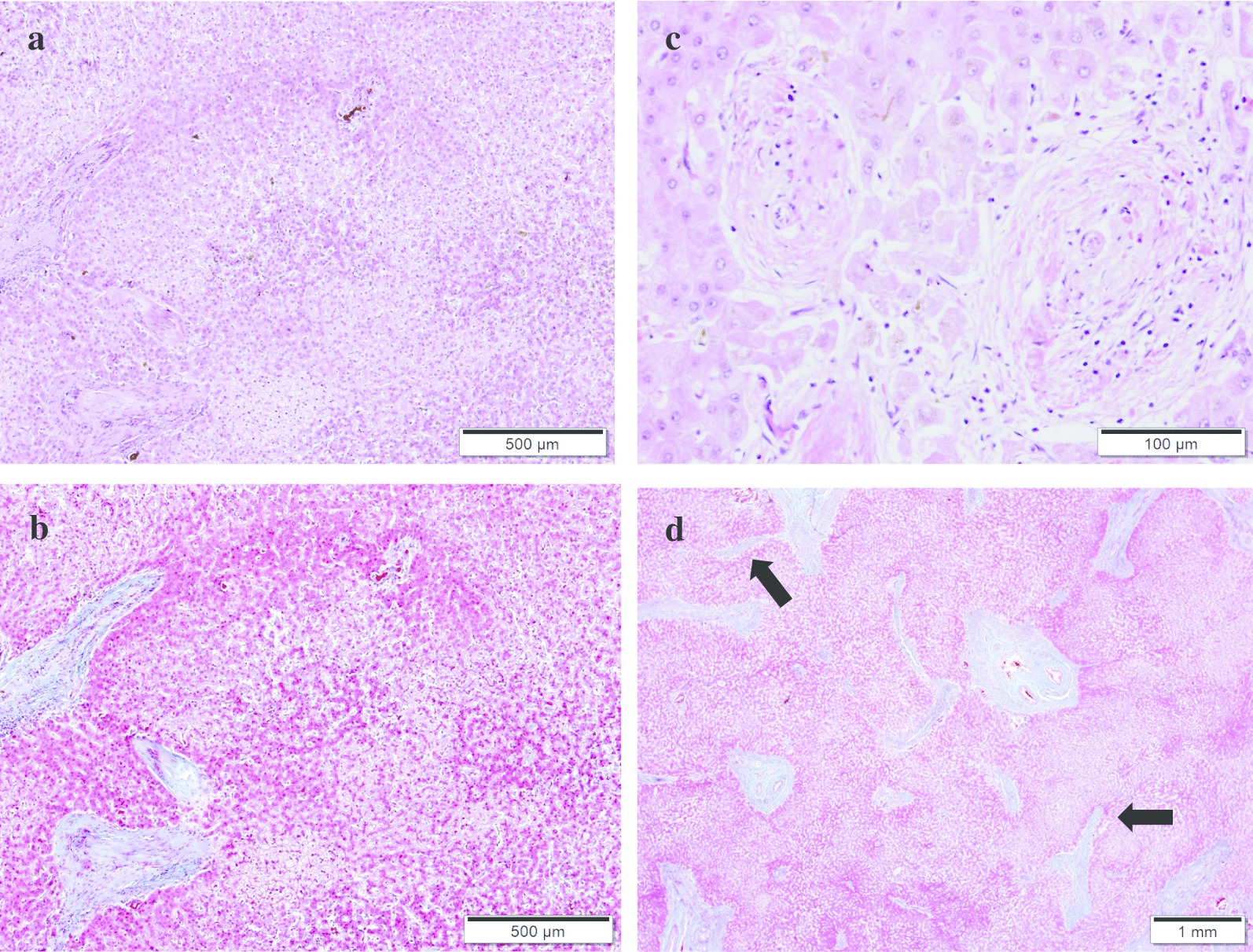
Case presentation: We report the case of a 51-year-old female patient diagnosed with IPH more than 20 years ago. She suffered severe jaundice, massive ascites, and encephalopathy at the time of her visit to our hospital. The patient's extrahepatic portal vein showed a scar-like stenosis, and the portal flow was completely hepatofugal. Collateral circulation such as the splenorenal shunt was well developed, and multiple splenic artery aneurysms up to 2 cm were observed in the splenic hilum. Her Model for End-Stage Liver Disease score increased to over 40 because of renal dysfunction, requiring temporary dialysis. We performed LDLT using her husband's right lobe graft and splenectomy. The extrahepatic stenotic portal vein was completely resected, and the superficial femoral vein (SFV) graft collected from the recipient's right leg was used for portal reconstruction as an interposition graft. Although the clinical course after LDLT had many complications, the patient was discharged on postoperative day 113 and has been fine for 2 years after LDLT. Histopathologically, the explanted liver had obliterative portal venopathy, nodular regenerative hyperplasia, and incomplete septal cirrhosis.
Conclusion: This case showed that severe IPH is occasionally associated with extrahepatic portal vein stenosis and can be treated with LDLT with portal vein reconstruction using an interposition graft. It was also suggested that the SFV is a useful choice for the interposition graft.
Keywords: Extrahepatic portal vein stenosis; Idiopathic portal hypertension; Living donor liver transplantation; Splenic artery aneurysms; Superficial femoral vein graft.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
