

Combining structured and unstructured data for predictive models: a deep learning approach
- PMID: 33121479
- PMCID: PMC7596962
- DOI: 10.1186/s12911-020-01297-6
Combining structured and unstructured data for predictive models: a deep learning approach
Abstract
Background: The broad adoption of electronic health records (EHRs) provides great opportunities to conduct health care research and solve various clinical problems in medicine. With recent advances and success, methods based on machine learning and deep learning have become increasingly popular in medical informatics. However, while many research studies utilize temporal structured data on predictive modeling, they typically neglect potentially valuable information in unstructured clinical notes. Integrating heterogeneous data types across EHRs through deep learning techniques may help improve the performance of prediction models.
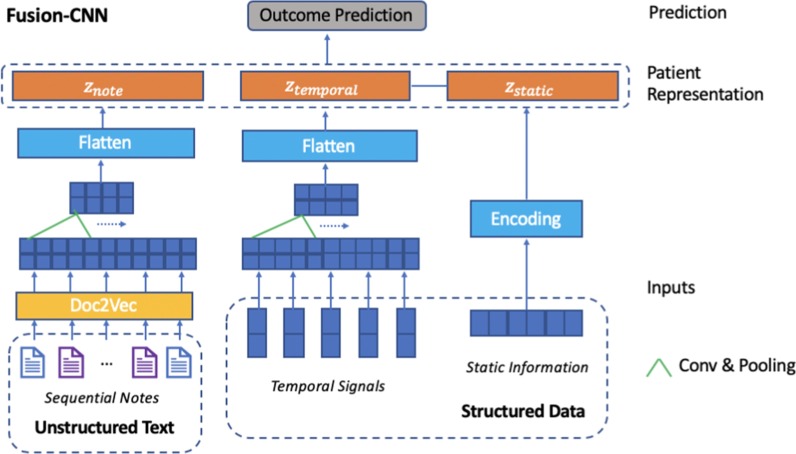
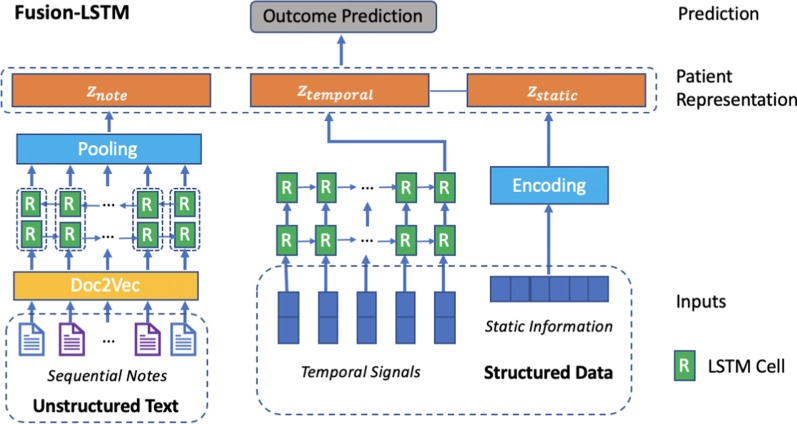
Methods: In this research, we proposed 2 general-purpose multi-modal neural network architectures to enhance patient representation learning by combining sequential unstructured notes with structured data. The proposed fusion models leverage document embeddings for the representation of long clinical note documents and either convolutional neural network or long short-term memory networks to model the sequential clinical notes and temporal signals, and one-hot encoding for static information representation. The concatenated representation is the final patient representation which is used to make predictions.
Results: We evaluate the performance of proposed models on 3 risk prediction tasks (i.e. in-hospital mortality, 30-day hospital readmission, and long length of stay prediction) using derived data from the publicly available Medical Information Mart for Intensive Care III dataset. Our results show that by combining unstructured clinical notes with structured data, the proposed models outperform other models that utilize either unstructured notes or structured data only.
Conclusions: The proposed fusion models learn better patient representation by combining structured and unstructured data. Integrating heterogeneous data types across EHRs helps improve the performance of prediction models and reduce errors.
Keywords: Data fusion; Deep learning; Electronic health records; Time series forecasting.
Conflict of interest statement
PZ is the member of the editorial board of BMC Medical Informatics and Decision Making. The authors declare that they have no other competing interests.
Figures
References
-
- Henry J, Pylypchuk Y, Searcy T, Patel V. Adoption of electronic health record systems among US non-federal acute care hospitals: 2008–2015. ONC Data Brief. 2016;35:1–9.
-
- Bisbal M, Jouve E, Papazian L, de Bourmont S, Perrin G, Eon B, et al. Effectiveness of SAPS III to predict hospital mortality for post-cardiac arrest patients. Resuscitation. 2014;85(7):939–944. - PubMed
-
- Zimmerman JE, Kramer AA, McNair DS, Malila FM. Acute Physiology and Chronic Health Evaluation (APACHE) IV: hospital mortality assessment for today’s critically ill patients. Crit Care Med. 2006;34(5):1297–1310. - PubMed
-
- Donzé J, Aujesky D, Williams D, Schnipper JL. Potentially avoidable 30-day hospital readmissions in medical patients: derivation and validation of a prediction model. JAMA Internal Med. 2013;173(8):632–638. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
