

Registry of Arterial and Venous Thromboembolic Complications in Patients With COVID-19
- PMID: 33121712
- PMCID: PMC7588178
- DOI: 10.1016/j.jacc.2020.08.070
Registry of Arterial and Venous Thromboembolic Complications in Patients With COVID-19
Abstract
Background: Cardiovascular complications, including myocardial infarction, ischemic stroke, and pulmonary embolism, represent an important source of adverse outcomes in coronavirus disease-2019 (COVID-19).
Objectives: To assess the frequency of arterial and venous thromboembolic disease, risk factors, prevention and management patterns, and outcomes in patients with COVID-19, the authors designed a multicenter, observational cohort study.
Methods: We analyzed a retrospective cohort of 1,114 patients with COVID-19 diagnosed through our Mass General Brigham integrated health network. The total cohort was analyzed by site of care: intensive care (n = 170); hospitalized nonintensive care (n = 229); and outpatient (n = 715). The primary study outcome was a composite of adjudicated major arterial or venous thromboembolism.
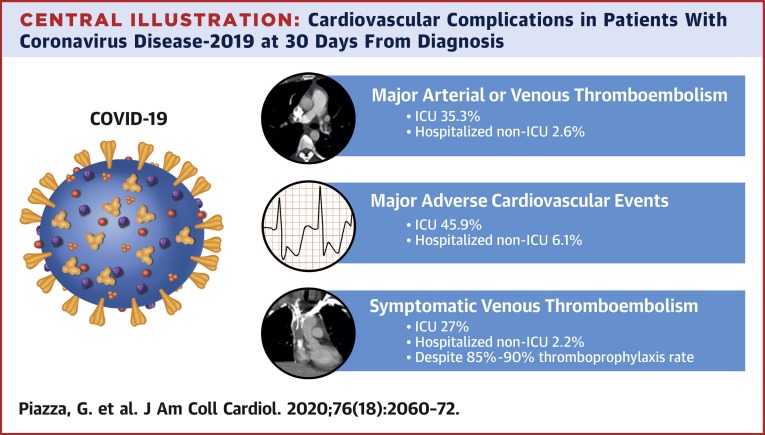
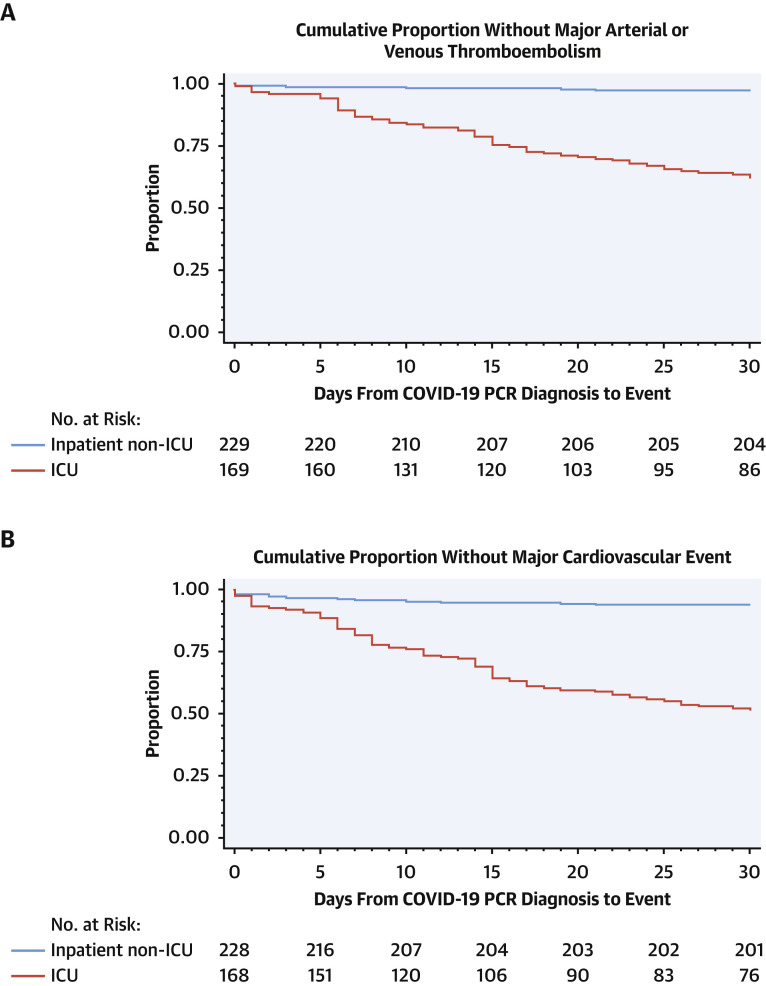
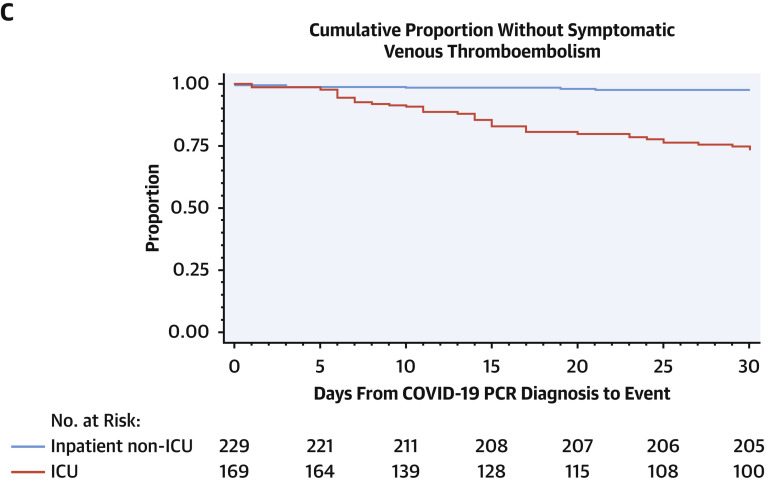
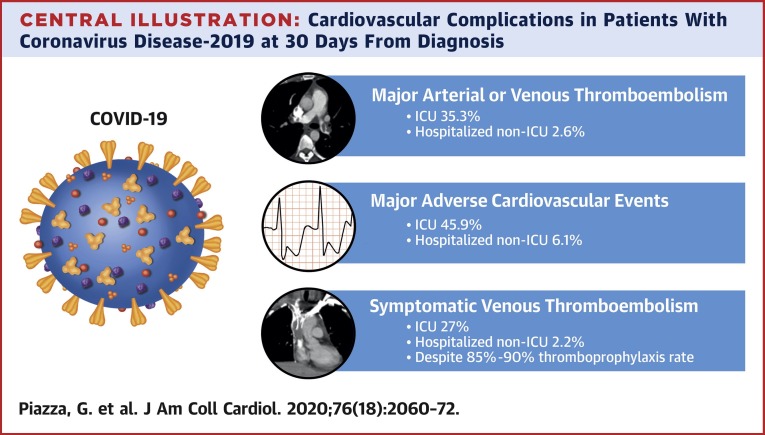
Results: Patients with COVID-19 were 22.3% Hispanic/Latinx and 44.2% non-White. Cardiovascular risk factors of hypertension (35.8%), hyperlipidemia (28.6%), and diabetes (18.0%) were common. Prophylactic anticoagulation was prescribed in 89.4% of patients with COVID-19 in the intensive care cohort and 84.7% of those in the hospitalized nonintensive care setting. Frequencies of major arterial or venous thromboembolism, major cardiovascular adverse events, and symptomatic venous thromboembolism were highest in the intensive care cohort (35.3%, 45.9%, and 27.0 %, respectively) followed by the hospitalized nonintensive care cohort (2.6%, 6.1%, and 2.2%, respectively) and the outpatient cohort (0% for all).
Conclusions: Major arterial or venous thromboembolism, major adverse cardiovascular events, and symptomatic venous thromboembolism occurred with high frequency in patients with COVID-19, especially in the intensive care setting, despite a high utilization rate of thromboprophylaxis.
Keywords: COVID-19; anticoagulation; cardiovascular disease; coronavirus; deep venous thrombosis; myocardial infarction; pulmonary embolism; stroke; thromboembolism.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Thromboembolism and the Pandemic.J Am Coll Cardiol. 2020 Nov 3;76(18):2073-2075. doi: 10.1016/j.jacc.2020.09.543. J Am Coll Cardiol. 2020. PMID: 33121713 Free PMC article.
References
-
- Bonow R.O., Fonarow G.C., O'Gara P.T., Yancy C.W. Association of coronavirus disease 2019 (COVID-19) with myocardial injury and mortality. JAMA Cardiol. 2020;5:751–753. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
