

doi: 10.3174/ajnr.A6844.
Epub 2020 Oct 29.
Decubitus CT Myelography for CSF-Venous Fistulas: A Procedural Approach
Affiliations
- PMID: 33122215
- PMCID: PMC7814789
- DOI: 10.3174/ajnr.A6844
Item in Clipboard
Decubitus CT Myelography for CSF-Venous Fistulas: A Procedural Approach
AJNR Am J Neuroradiol.
2021 Jan.
Abstract
Decubitus CT myelography is a reported method to identify CSF-venous fistulas in patients with spontaneous intracranial hypotension. One of the main advantages of decubitus CT myelography in detecting CSF-venous fistulas is using gravity to dependently opacify the CSF-venous fistula, which can be missed on traditional myelographic techniques. Most of the CSF-venous fistulas in the literature have been identified in patients receiving general anesthesia and digital subtraction myelography, a technique that is not performed at all institutions. In this article, we discuss the decubitus CT myelography technique and how to implement it in daily practice.
© 2021 by American Journal of Neuroradiology.
Figures
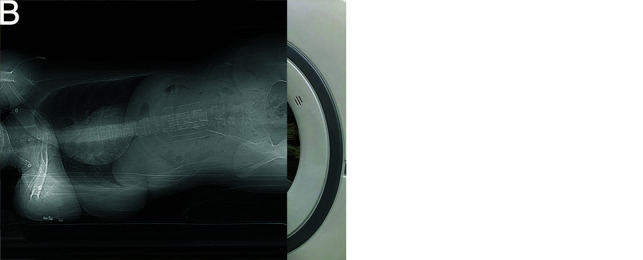
Patient positioning for decubitus CTM. A, A custom-made firm wedge with a 20° angle is placed on the CT gantry, and the hips are placed at the apex of the wedge with the feet closest to the scanner bore. If no wedge is available, 1–2 pillows can be placed instead. Pillows can also be used to support the legs. B, A lateral scout radiograph shows an adequate angle to facilitate contrast transit from the lumbar puncture to the remainder of the spine.
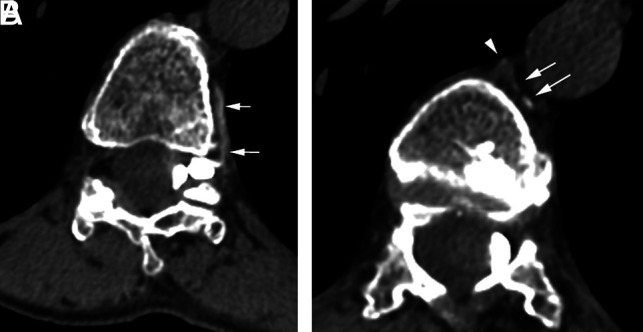
A CSF-venous fistula on decubitus CTM. A, Axial left-decubitus CTM shows a paravertebral vein (arrows) arising from a large left meningeal diverticulum at the T11–T12 level. B, On a more superior section, the vein (arrows) drains into the azygous vein (arrowhead).

Value of decubitus CTM in diagnosing a CSF-venous fistula. A, An axial conventional CTM at the T10–T11 level shows bilateral meningeal diverticula without evidence of a CSF-venous fistula. B, An axial MR imaging myelogram with intrathecal gadolinium shows similar findings. C, A right-decubitus CTM in the axial oblique plane shows a right-sided CSF-venous fistula with a paravertebral course (arrows).

CSF-venous fistula on decubitus CT and intrathecal MR imaging myelograms. A, An axial conventional CTM shows a large, irregular right meningeal diverticulum at the T8–T9 level but no abnormal vein. B, An axial right-decubitus CTM shows a CSF-venous fistula (arrows). C, An axial MR imaging myelogram with intrathecal gadolinium faintly shows the CSF-venous fistula (arrow), but it is not as apparent as the decubitus CTM.

Importance of immediate scanning in decubitus CTM. A, An axial right-decubitus CTM scanned immediately after contrast injection shows abnormal veins (arrows) arising from a large right meningeal diverticulum at the L1–L2 level. B, On a more superior section, the vein (arrows) has a paravertebral course and terminates in the vertebral body. C, An axial right-decubitus CTM from a 3-minute delayed scan shows absence of the abnormal veins. If it were not for the initial scan, the CSF-venous fistula would have not been detected.

Value of precontrast imaging in a 39 year-old-man with a nearly 20-year history of SIH. Ten years previously, the patient underwent surgical removal of a spinal venous malformation in the T1 posterior elements and dorsal epidural space, which was causing cord compression (not shown). A, An axial conventional CTM shows a round hyperdense focus in the right, lateral epidural space (arrow) and a broad hyperdense structure in the dorsal epidural space (arrowheads) at the T2–T3 level. This was suspicious for a CSF-venous fistula, but in the context of the surgical fusion, it was unclear whether the dorsal epidural hyperdensity was postsurgical. In the same session as the decubitus CTM, noncontrast imaging of the upper thoracic spine (B) was performed, which confirmed that the dorsal epidural hyperdensity (arrow) was postsurgical. C, An axial oblique CT image from a right-decubitus CTM shows a large CSF-venous fistula (arrows) at the T1–T2 level, which is most likely associated with the prior venous malformation.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical