

Association of Multiple Plasma Biomarker Concentrations with Progression of Prevalent Diabetic Kidney Disease: Findings from the Chronic Renal Insufficiency Cohort (CRIC) Study
- PMID: 33122288
- PMCID: PMC7894671
- DOI: 10.1681/ASN.2020040487
Association of Multiple Plasma Biomarker Concentrations with Progression of Prevalent Diabetic Kidney Disease: Findings from the Chronic Renal Insufficiency Cohort (CRIC) Study
Abstract
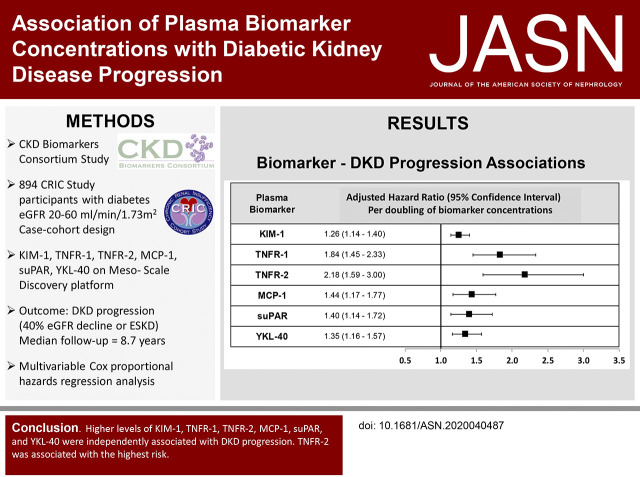
Background: Although diabetic kidney disease is the leading cause of ESKD in the United States, identifying those patients who progress to ESKD is difficult. Efforts are under way to determine if plasma biomarkers can help identify these high-risk individuals.
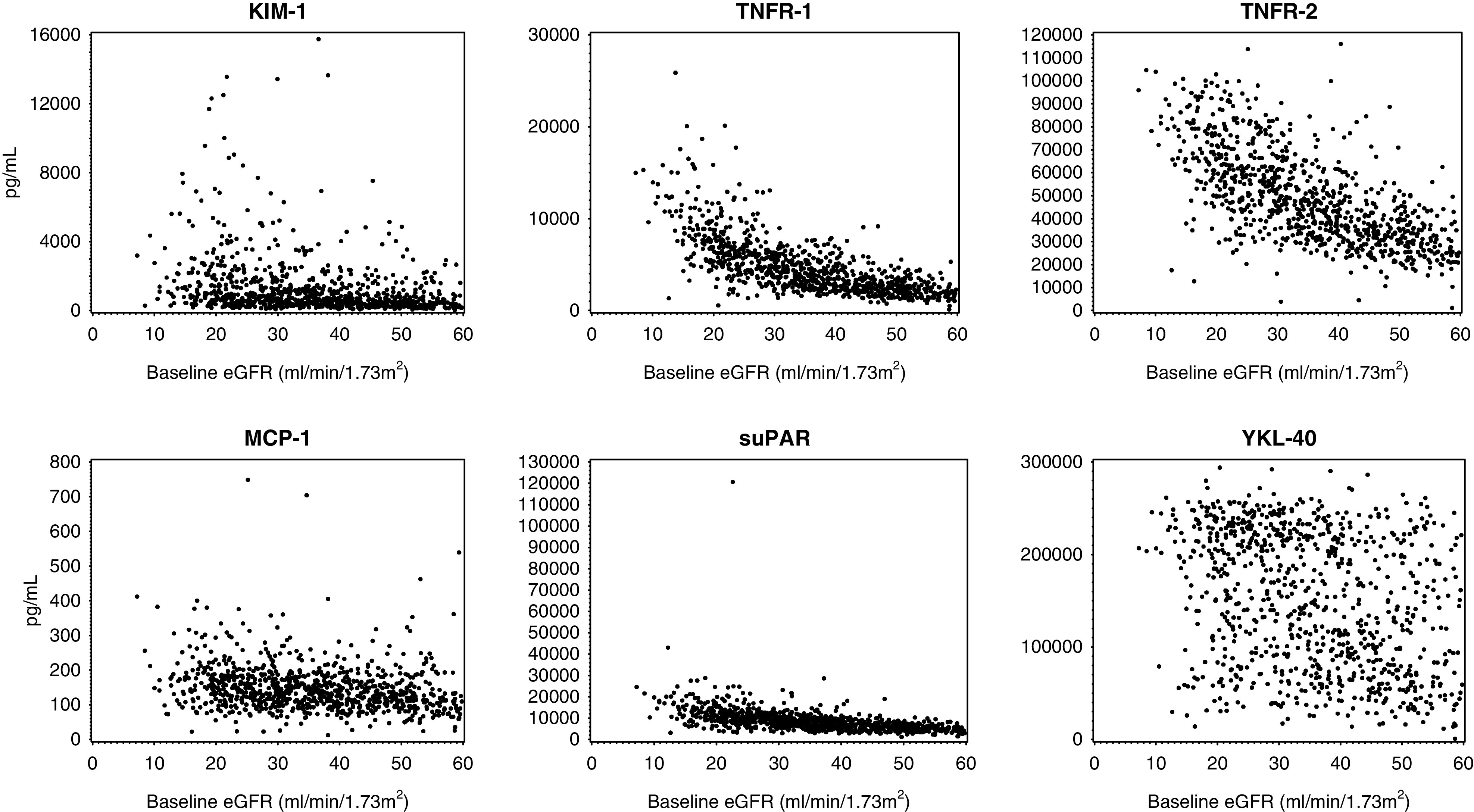
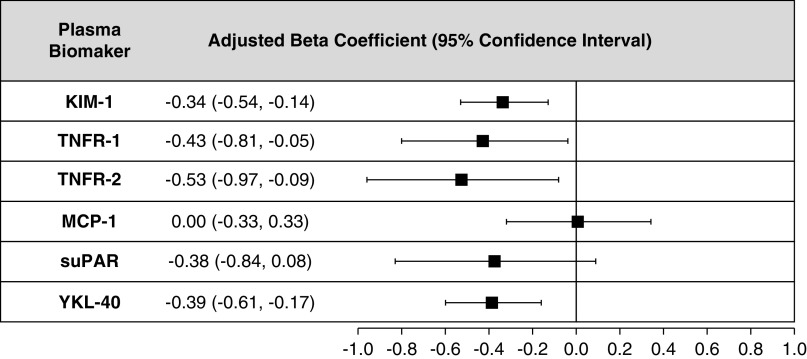
Methods: In our case-cohort study of 894 Chronic Renal Insufficiency Cohort Study participants with diabetes and an eGFR of <60 ml/min per 1.73 m2 at baseline, participants were randomly selected for the subcohort; cases were those patients who developed progressive diabetic kidney disease (ESKD or 40% eGFR decline). Using a multiplex system, we assayed plasma biomarkers related to tubular injury, inflammation, and fibrosis (KIM-1, TNFR-1, TNFR-2, MCP-1, suPAR, and YKL-40). Weighted Cox regression models related biomarkers to progression of diabetic kidney disease, and mixed-effects models estimated biomarker relationships with rate of eGFR change.
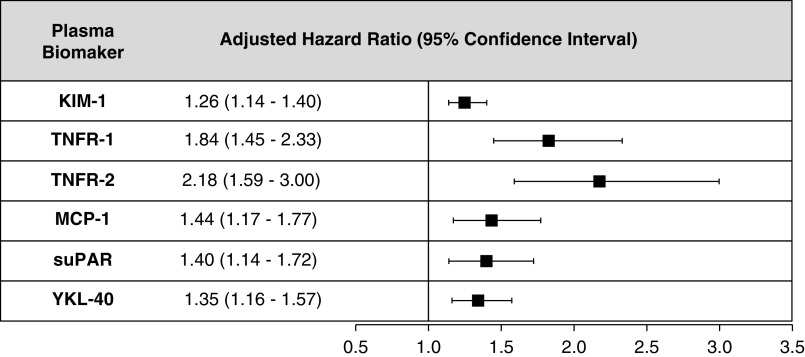
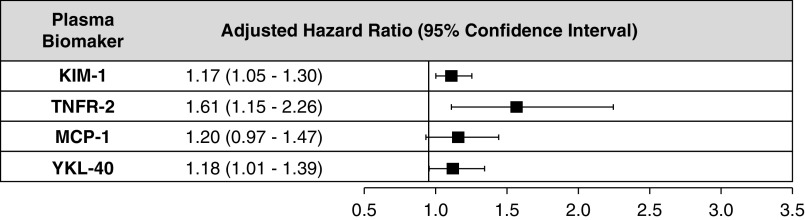
Results: Median follow-up was 8.7 years. Higher concentrations of KIM-1, TNFR-1, TNFR-2, MCP-1, suPAR, and YKL-40 were each associated with a greater risk of progression of diabetic kidney disease, even after adjustment for established clinical risk factors. After accounting for competing biomarkers, KIM-1, TNFR-2, and YKL-40 remained associated with progression of diabetic kidney disease; TNFR-2 had the highest risk (adjusted hazard ratio, 1.61; 95% CI, 1.15 to 2.26). KIM-1, TNFR-1, TNFR-2, and YKL-40 were associated with rate of eGFR decline.
Conclusions: Higher plasma levels of KIM-1, TNFR-1, TNFR-2, MCP-1, suPAR, and YKL-40 were associated with increased risk of progression of diabetic kidney disease; TNFR-2 had the highest risk after accounting for the other biomarkers. These findings validate previous literature on TNFR-1, TNFR-2, and KIM-1 in patients with prevalent CKD and provide new insights into the influence of suPAR and YKL-40 as plasma biomarkers that require validation.
Keywords: biomarker; chronic diabetic complications; chronic kidney disease; diabetes; diabetic kidney disease; diabetic nephropathy; end stage kidney disease; epidemiology and outcomes.
Copyright © 2021 by the American Society of Nephrology.
Figures
References
-
- Reutens AT: Epidemiology of diabetic kidney disease. Med Clin North Am 97: 1–18, 2013. - PubMed
-
- United States Renal Data System (USRDS) : Chapter 1: Incidence, prevalence, patient characteristics, and treatment modalities. Available at: https://www.usrds.org/media/1688/v2_c01_incprev_17.pdf. Accessed June 20, 2019
-
- Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR; UKPDS Study Group : Risk factors for renal dysfunction in type 2 diabetes: U.K. prospective diabetes study 74. Diabetes 55: 1832–1839, 2006. - PubMed
-
- Porrini E, Ruggenenti P, Luis-Lima S, Carrara F, Jiménez A, de Vries APJ, et al. .: Estimated GFR: Time for a critical appraisal. Nat Rev Nephrol 15: 177–190, 2019. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UL1 TR000424/TR/NCATS NIH HHS/United States
- UL1 TR002548/TR/NCATS NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- R01 HL085757/HL/NHLBI NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- R01 DK112258/DK/NIDDK NIH HHS/United States
- R01 DK104730/DK/NIDDK NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- K08 DK110536/DK/NIDDK NIH HHS/United States
- U01 DK085660/DK/NIDDK NIH HHS/United States
- R01 DK115562/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- K01 DK107782/DK/NIDDK NIH HHS/United States
- K23 DK118198/DK/NIDDK NIH HHS/United States
- R21 HL143089/HL/NHLBI NIH HHS/United States
- U01 DK106962/DK/NIDDK NIH HHS/United States
- U01 DK102730/DK/NIDDK NIH HHS/United States
- P30 DK079626/DK/NIDDK NIH HHS/United States
- U01 DK103225/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- R37 DK039773/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- L40 DK110937/DK/NIDDK NIH HHS/United States
- R01 DK119199/DK/NIDDK NIH HHS/United States
- U01OH011326/ACL/ACL HHS/United States
- U01 DK106965/DK/NIDDK NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- L30 DK110819/DK/NIDDK NIH HHS/United States
- U01 OH011326/OH/NIOSH CDC HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
