

Managing drug-induced QT prolongation in clinical practice
- PMID: 33122341
- PMCID: PMC8237186
- DOI: 10.1136/postgradmedj-2020-138661
Managing drug-induced QT prolongation in clinical practice
Abstract
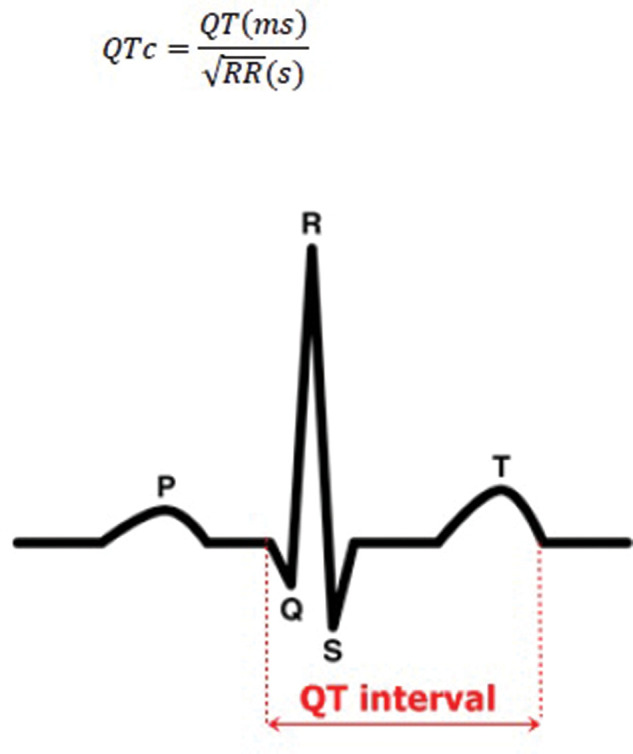
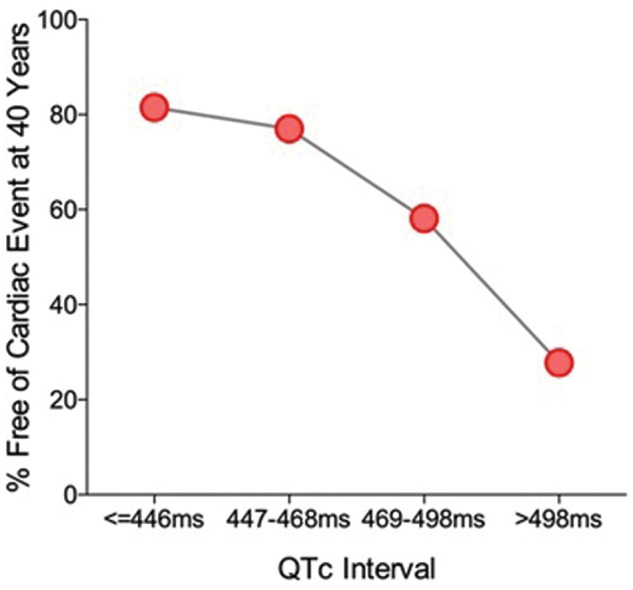
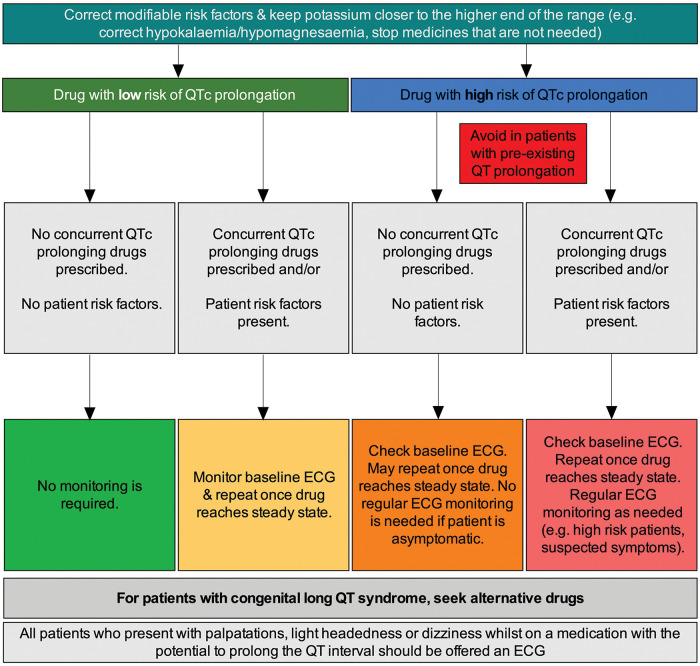
Many drug therapies are associated with prolongation of the QT interval. This may increase the risk of Torsades de Pointes (TdP), a potentially life-threatening cardiac arrhythmia. As the QT interval varies with a change in heart rate, various formulae can adjust for this, producing a 'corrected QT' (QTc) value. Normal QTc intervals are typically <450 ms for men and <460 ms for women. For every 10 ms increase, there is a ~5% increase in the risk of arrhythmic events. When prescribing drugs associated with QT prolongation, three key factors should be considered: patient-related risk factors (eg, female sex, age >65 years, uncorrected electrolyte disturbances); the potential risk and degree of QT prolongation associated with the proposed drug; and co-prescribed medicines that could increase the risk of QT prolongation. To support clinicians, who are likely to prescribe such medicines in their daily practice, we developed a simple algorithm to help guide clinical management in patients who are at risk of QT prolongation/TdP, those exposed to QT-prolonging medication or have QT prolongation.
Keywords: Adverse events; Cardiology; Clinical pharmacology; Pacing & electrophysiology; Therapeutics.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
