

Augmented reality improves procedural efficiency and reduces radiation dose for CT-guided lesion targeting: a phantom study using HoloLens 2
- PMID: 33122766
- PMCID: PMC7596500
- DOI: 10.1038/s41598-020-75676-4
Augmented reality improves procedural efficiency and reduces radiation dose for CT-guided lesion targeting: a phantom study using HoloLens 2
Abstract
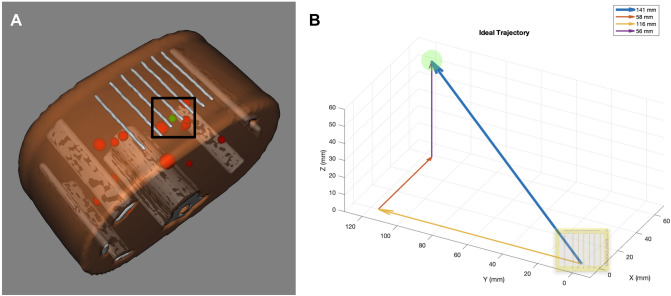
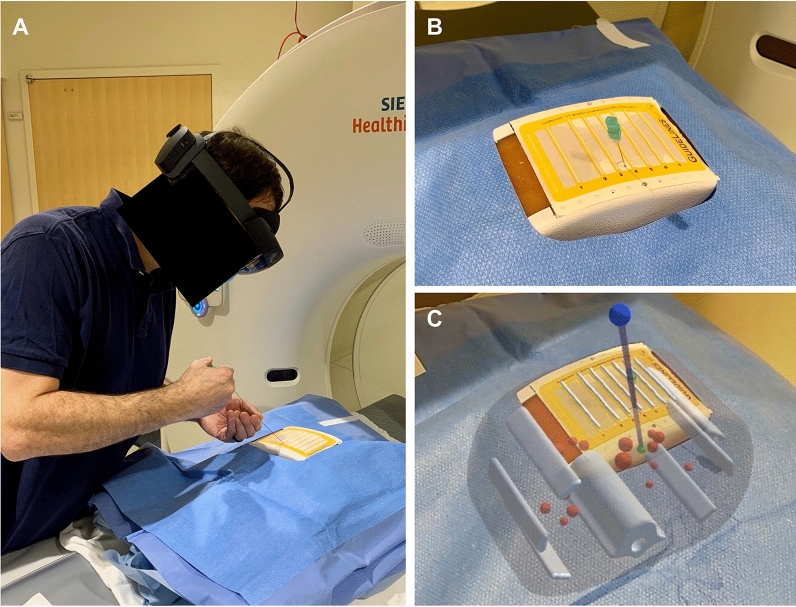
Out-of-plane lesions pose challenges for CT-guided interventions. Augmented reality (AR) headsets are capable to provide holographic 3D guidance to assist CT-guided targeting. A prospective trial was performed assessing CT-guided lesion targeting on an abdominal phantom with and without AR guidance using HoloLens 2. Eight operators performed a cumulative total of 86 needle passes. Total needle redirections, radiation dose, procedure time, and puncture rates of nontargeted lesions were compared with and without AR. Mean number of needle passes to reach the target reduced from 7.4 passes without AR to 3.4 passes with AR (p = 0.011). Mean CT dose index decreased from 28.7 mGy without AR to 16.9 mGy with AR (p = 0.009). Mean procedure time reduced from 8.93 min without AR to 4.42 min with AR (p = 0.027). Puncture rate of a nontargeted lesion decreased from 11.9% without AR (7/59 passes) to 0% with AR (0/27 passes). First needle passes were closer to the ideal target trajectory with AR versus without AR (4.6° vs 8.0° offset, respectively, p = 0.018). AR reduced variability and elevated the performance of all operators to the same level irrespective of prior clinical experience. AR guidance can provide significant improvements in procedural efficiency and radiation dose savings for targeting out-of-plane lesions.
Conflict of interest statement
The authors declare no competing interests.
Figures




References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
