

Reduced Environmental Stimulation in Anorexia Nervosa: An Early-Phase Clinical Trial
- PMID: 33123048
- PMCID: PMC7573249
- DOI: 10.3389/fpsyg.2020.567499
Reduced Environmental Stimulation in Anorexia Nervosa: An Early-Phase Clinical Trial
Abstract
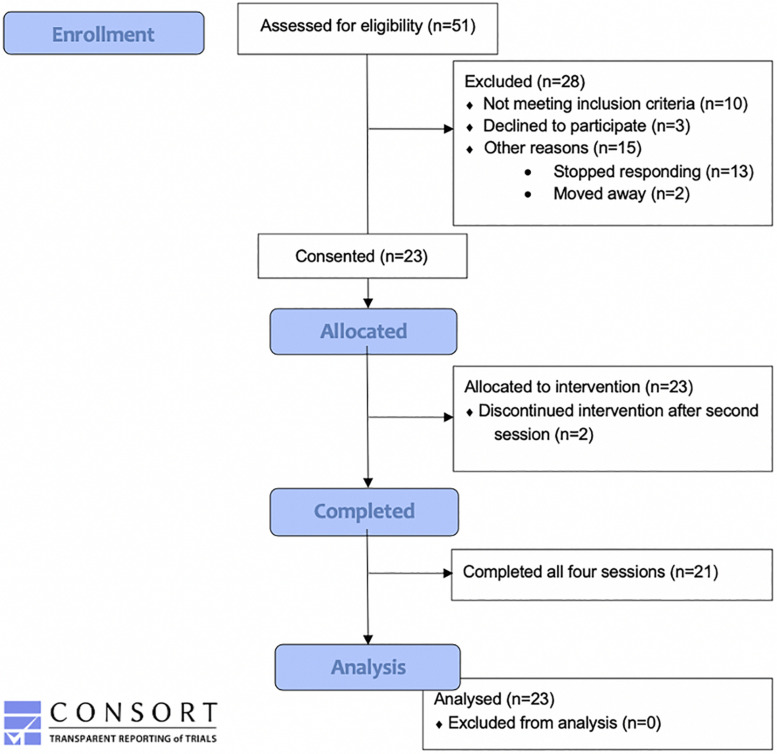
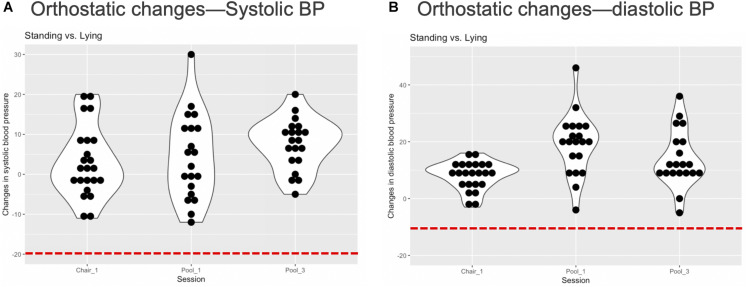
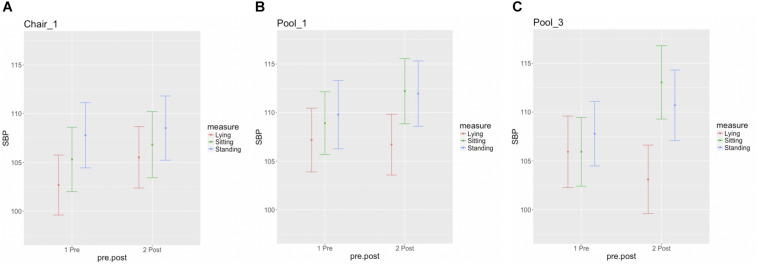
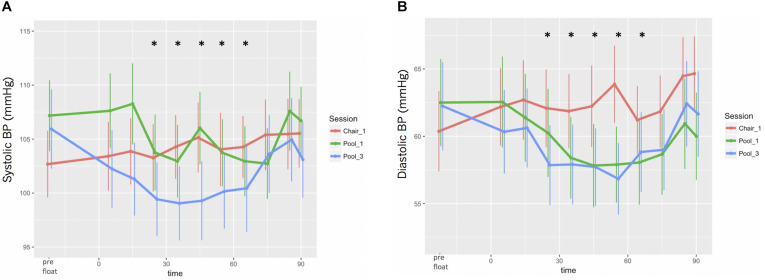
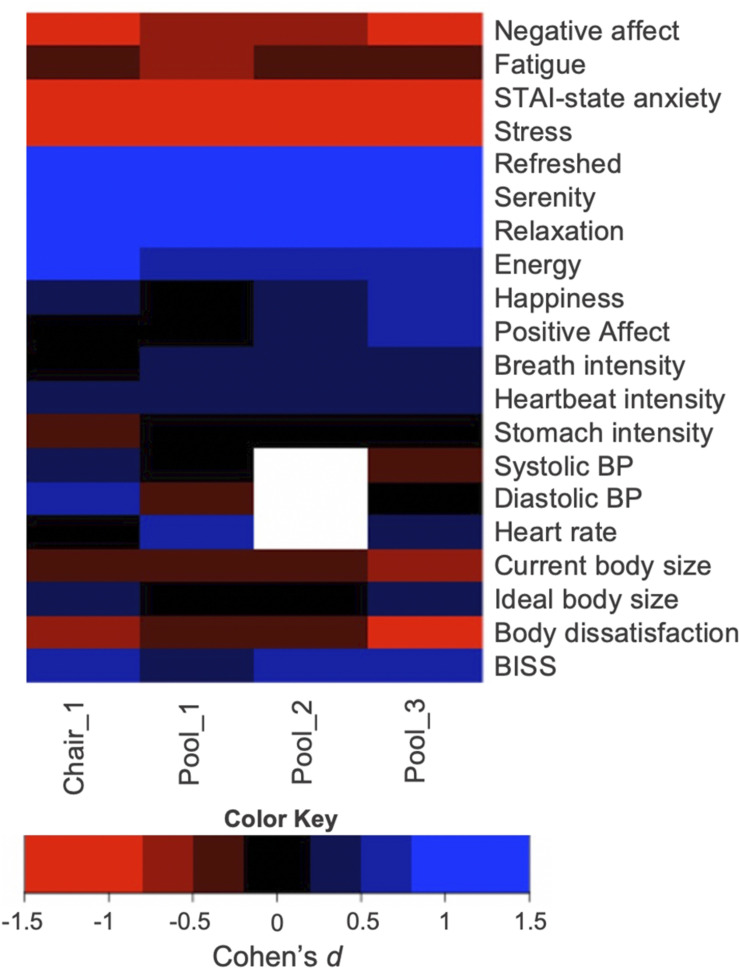
Reduced Environmental Stimulation Therapy (REST) alters the balance of sensory input to the nervous system by systematically attenuating sensory signals from visual, auditory, thermal, tactile, vestibular, and proprioceptive channels. Previous research from our group has shown that REST via floatation acutely reduces anxiety and blood pressure (BP) while simultaneously heightening interoceptive awareness in clinically anxious populations. Anorexia nervosa (AN) is an eating disorder characterized by elevated anxiety, distorted body representation, and abnormal interoception, raising the question of whether REST might positively impact these symptoms. However, this approach has never been studied in eating disorders, and it is unknown whether exposure to floatation REST might worsen AN symptoms. To examine these possibilities, we conducted an open-label study to investigate the safety and tolerability of REST in AN. We also explored the acute impact of REST on BP, affective symptoms, body image disturbance, and interoception. Twenty-one partially weight-restored AN outpatients completed a protocol involving four sequential sessions of REST: reclining in a zero-gravity chair, floating in an open pool, and two sessions of floating in an enclosed pool. All sessions were 90 min, approximately 1 week apart. We measured orthostatic BP before and immediately after each session (primary outcome), in addition to collecting BP readings every 10 min during the session using a wireless waterproof system as a secondary outcome measure. Each participant's affective state, awareness of interoceptive sensations, and body image were assessed before and after every session (exploratory outcomes). There was no evidence of orthostatic hypotension following floating, and no adverse events (primary outcome). Secondary analyses revealed that REST induced statistically significant reductions in BP (p < 0.001; Cohen's d, 0.2-0.5), anxiety (p < 0.001; Cohen's d, >1) and negative affect (p < 0.01; Cohen's d, >0.5), heightened awareness of cardiorespiratory (p < 0.01; Cohen's d, 0.2-0.5) but not gastrointestinal sensations, and reduced body image dissatisfaction (p < 0.001; Cohen's d, >0.5). The findings from this initial trial suggest that individuals with AN can safely tolerate the physical effects of REST via floatation. Future randomized controlled trials will need to investigate whether these initial observations of improved anxiety, interoception, and body image disturbance occur in acutely ill AN populations.
Clinical trial registration: ClinicalTrials.gov; Identifier: NCT02801084 (April 01, 2016).
Keywords: body awareness; body image; eating disorder; floatation therapy; interoception; interoceptive awareness; stress.
Copyright © 2020 Khalsa, Moseman, Yeh, Upshaw, Persac, Breese, Lapidus, Chappelle, Paulus and Feinstein.
Figures


References
-
- American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: American Psychiatric Association.
-
- Barabasz M. (1993). “REST: a key facilitator in the treatment of eating disorders,” in Clinical and Experimental Restricted Environmental Stimulation: New Developments and Perspectives, eds Barabasz A. F., Barabasz M. (New York, NY: Springer-Verlag; ), 121–126. 10.1007/978-1-4684-8583-7_15 - DOI
-
- Bates D., Maechler M., Boker B., Walker S. (2015). Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67 1–48.
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous