

The Association Between Obesity and Risk of Acute Kidney Injury After Cardiac Surgery
- PMID: 33123083
- PMCID: PMC7573233
- DOI: 10.3389/fendo.2020.534294
The Association Between Obesity and Risk of Acute Kidney Injury After Cardiac Surgery
Abstract
Objective: To determine the relationship between obesity and the risk of AKI after cardiac surgery (CS-AKI) in a cohort study.
Methods: A total of 1,601 patients undergoing cardiac surgery were collected and their incidence of CS-AKI was recorded. They were divided into underweight, normal weight, overweight, and obese groups. Logistic regression was used to estimate the association between BMI (body mass index) and CS-AKI risk. Then, a meta-analysis of published cohort studies was conducted to confirm this result using PubMed and Embase databases.
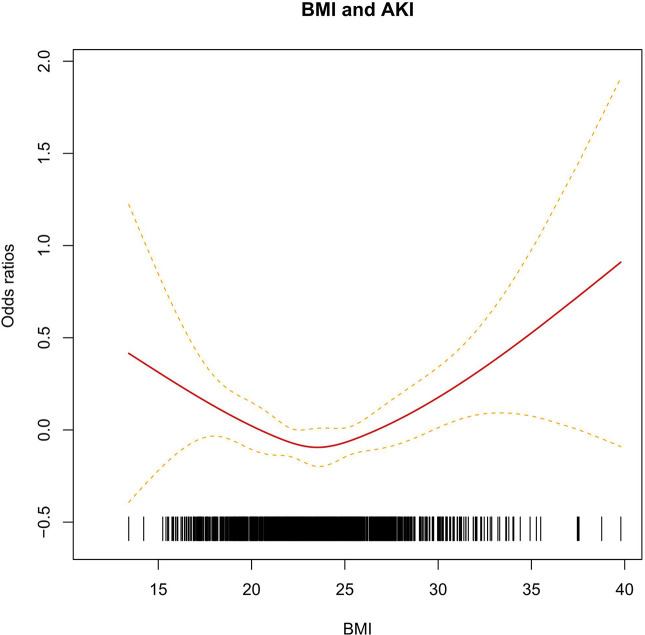
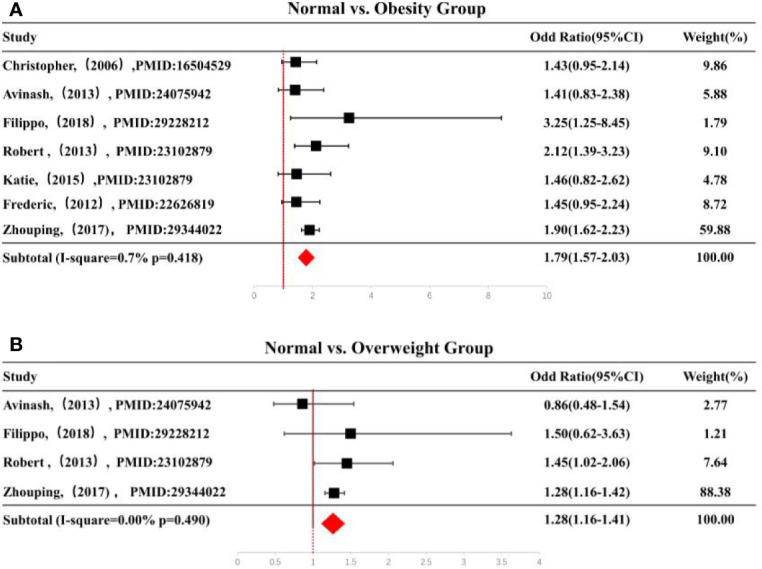
Results: A significant association was observed in this independent cohort after adjusting age, gender, hypertension and New York Heart Association classification (NYHA) class. Compared with normal BMI group (18.5 ≤ BMI < 24.0), the individuals with aberrant BMI level had an increased AKI risk (OR: 1.68, 95% CI: 1.01-2.78) for BMI < 18.5 group and (OR: 1.43, 95% CI: 0.96-2.15) for BMI ≥ 28.0. Interestingly, the U-shape curve showed the CS-AKI risk reduced with the increasing of BMI when BMI ≤ 24.0. As BMI increases with BMI > 24.0, the risk of developing CS-AKI increased significantly. In the confirmed meta-analysis, compared with normal weight, overweight group with cardiac surgery had higher AKI risk (OR: 1.28, 95% CI: 1.16-1.41, Pheterogeneity = 0.49). The similar association was found in obesity subgroup (OR: 1.79, 95% CI: 1.57-2.03, Pheterogeneity = 0.42).
Conclusion: In conclusion, the results suggested that abnormal BMI was a risk factor for CS-AKI independently.
Keywords: acute kidney injury; body mass index; cardiac surgery; creatinine; obesity.
Copyright © 2020 Shi, Liu, Fan, Yang, Zhang, Li, Wu, Li, Mao, Xu, Ma, Xiao and Jiang.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials