

SGLT2 inhibitors for non-diabetic kidney disease: drugs to treat CKD that also improve glycaemia
- PMID: 33123352
- PMCID: PMC7577767
- DOI: 10.1093/ckj/sfaa198
SGLT2 inhibitors for non-diabetic kidney disease: drugs to treat CKD that also improve glycaemia
Abstract
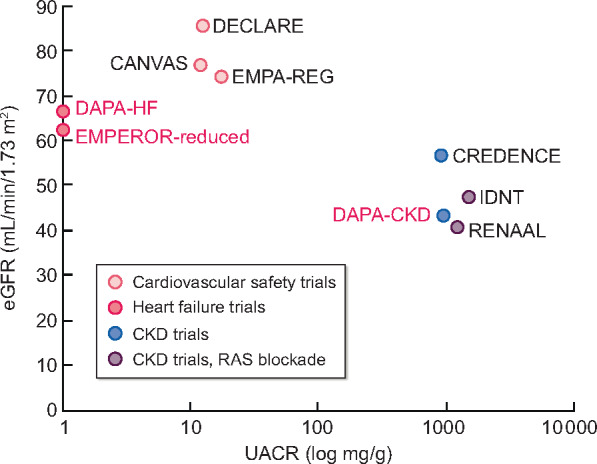
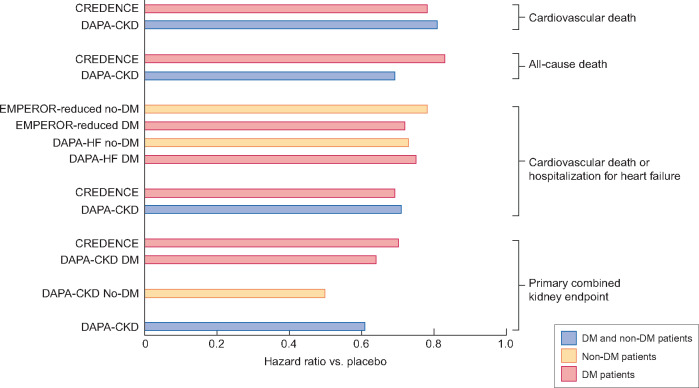
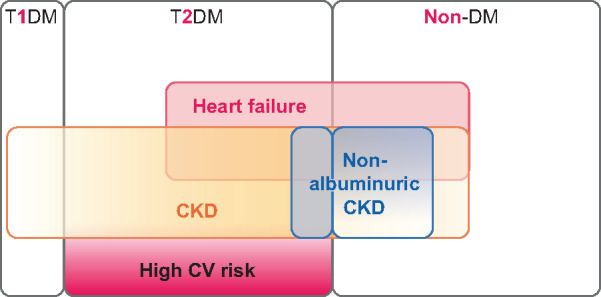
Sodium-glucose co-transporter-2 (SGLT2) inhibitors decreased cardiovascular (CV) events and improved renal outcomes in CV safety studies in type 2 diabetes melitus (T2DM) patients at high CV risk. Canagliflozin also improved kidney outcomes in diabetic kidney disease in the Canagliflozin and Renal Events in Diabetes and Nephropathy Clinical Evaluationtrial. More recently, the Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure (DAPA-HF) trial showed that dapagliflozin improved CV outcomes in patients with HF with or without diabetes. Protection from HF in non-diabetics was confirmed for empagliflozin in the EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction (EMPEROR-Reduced) trial. A meta-analysis of DAPA-HF and EMPEROR-Reduced confirmed reductions in all-cause and CV death and the combined risk of CV death or worsening HF, as well as in the composite renal endpoint {hazard ratio [HR] 0.62 [95% confidence interval (CI) 0.43-0.90]} without differences based on the presence of diabetes or baseline estimated glomerular filtration rate (eGFR). Moreover, the Study to Evaluate the Effect of Dapagliflozin on Renal Outcomes and Cardiovascular Mortality in Patients With Chronic Kidney Disease (DAPA-CKD) showed that dapagliflozin as an add-on over renin-angiotensin system blockade in patients with chronic kidney disease (CKD; with or without T2DM) reduced the HR for the primary endpoint (time to the first occurrence of ≥50% eGFR decline, end-stage kidney disease or renal or CV death) to 0.61 (95% CI 0.51-0.72) and for the secondary endpoints of worsening renal function or death from kidney failure [HR 0.56 (95% CI 0.45-0.68)], hospitalization for HF or CV death [HR 0.71 (95% CI 0.55-0.92)] and all-cause mortality [HR 0.69 (95% CI 0.53-0.88)]. These beneficial effects were consistent in patients with and without T2DM. In conclusion, SGLT2 inhibitors offer CV and kidney protection in both diabetic and non-diabetic CKD and, additionally, improve glycaemic control in T2DM, making them first-line therapy for CKD independent from diabetic status.
Keywords: SGLT2 inhibitor; chronic kidney disease; clinical trials; mortality; outcomes.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Ortiz A, Sanchez-Niño MD, Crespo-Barrio M. et al. The Spanish Society of Nephrology (SENEFRO) commentary to the Spain GBD 2016 report: keeping chronic kidney disease out of sight of health authorities will only magnify the problem. Nefrologia 2019; 39: 29–34 - PubMed
-
- Ferreira JP, Butler J, Rossignol P. et al. Abnormalities of potassium in heart failure: JACC state-of-the-art review. J Am Coll Cardiol 2020; 75: 2836–2850 - PubMed
-
- Sarafidis P, Ferro CJ, Morales E. et al. SGLT-2 inhibitors and GLP-1 receptor agonists for nephroprotection and cardioprotection in patients with diabetes mellitus and chronic kidney disease. A consensus statement by the EURECA-m and the DIABESITY working groups of the ERA-EDTA. Nephrol Dial Transplant 2019; 34: 208–230 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
