

Contemporary management of anaemia, erythropoietin resistance and cardiovascular risk in patients with advanced chronic kidney disease: a nationwide analysis
- PMID: 33123358
- PMCID: PMC7577763
- DOI: 10.1093/ckj/sfaa054
Contemporary management of anaemia, erythropoietin resistance and cardiovascular risk in patients with advanced chronic kidney disease: a nationwide analysis
Abstract
Background: Optimal management of chronic kidney disease (CKD) anaemia remains controversial and few studies have evaluated real-world management of anaemia in advanced CKD in the context of guideline recommendations.
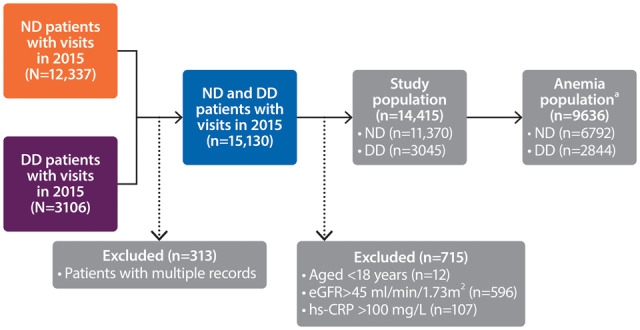
Methods: We performed an observational study from the Swedish Renal Registry evaluating the epidemiology and treatment patterns of anaemia across Stages 3b-5 in non-dialysis (ND) and dialysis-dependent (DD) CKD patients during 2015. Logistic regression and Cox models explored the associations between anaemia treatments, inflammation, erythropoietin resistance index (ERI) and subsequent 1-year risk of major adverse cardiovascular events (MACEs).
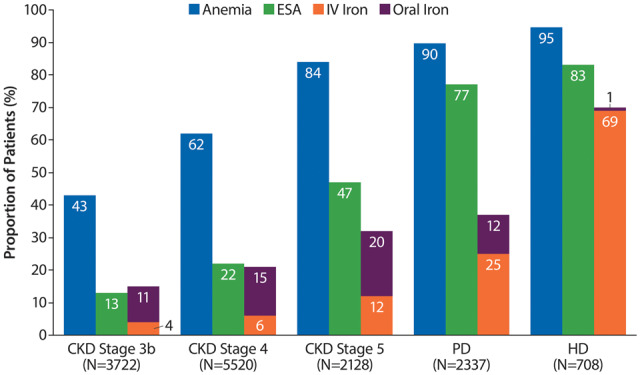
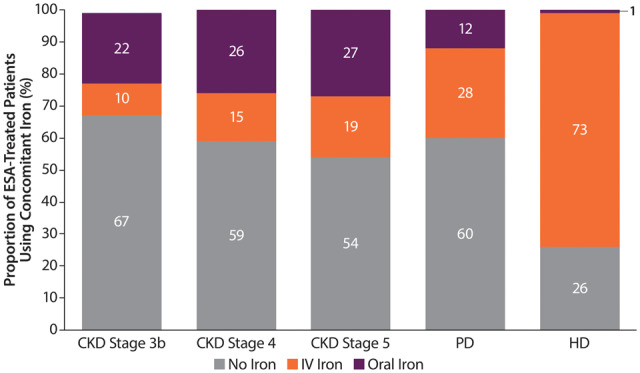
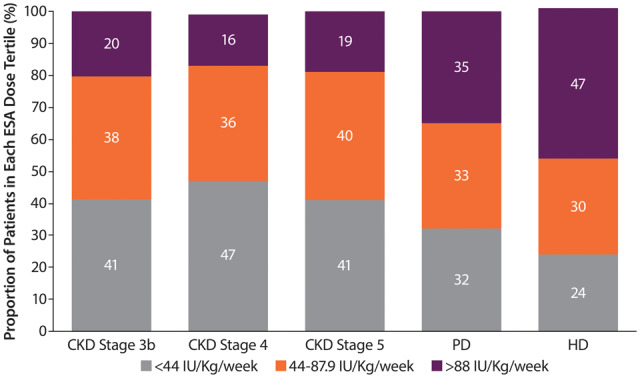
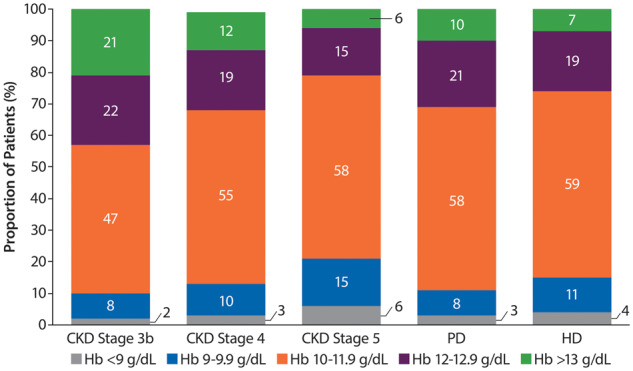
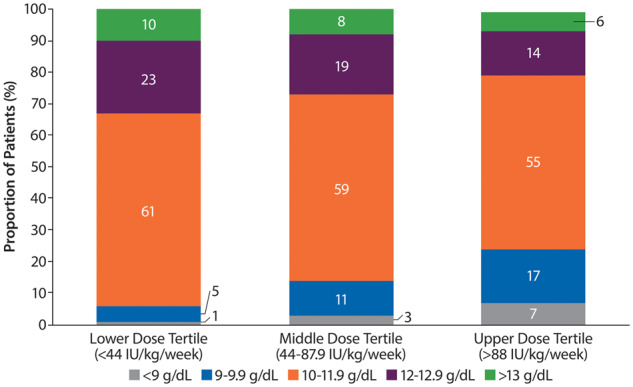
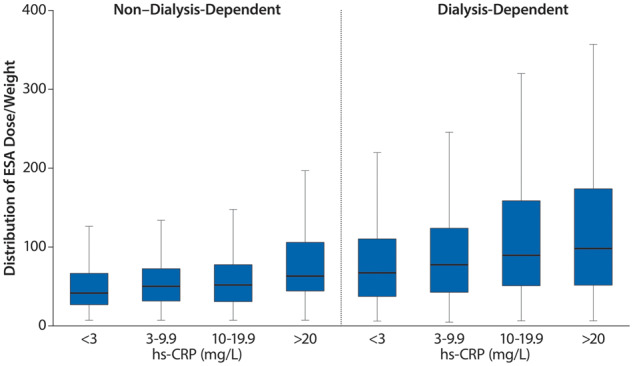
Results: Data from 14 415 (ND, 11 370; DD, 3045) patients were included. Anaemia occurred in 60% of ND and 93% of DD patients. DD patients used more erythropoiesis-stimulating agents (ESAs; 82% versus 24%) and iron (62% versus 21%) than ND patients. All weekly ESA doses were converted to a weight-adjusted weekly epoetin equivalent dose. The prescribed ESA doses were low to moderate [median 48.2 IU/kg/week (ND), 78.6 IU/kg/week (DD)]. Among ESA-treated patients, 6-21% had haemoglobin (Hb) >13 g/dL and 2-6% had Hb <9 g/dL. Inflammation (C-reactive protein >5 mg/L) was highly prevalent and associated with ERI and higher ESA doses. Higher (>88 IU/kg/week) versus lower (<44 IU/kg/week) ESA doses were associated with a higher risk of MACEs [{ND hazard ratio [HR] 1.36 [95% confidence interval (CI) 1.00-1.86]; DD HR 1.60 [95% CI 1.24-2.06]}. There was no association between iron use and inflammation or MACEs.
Conclusions: Anaemia remains highly prevalent in advanced CKD. Patients with anaemia received moderate ESA doses with a relatively low prevalence of iron use. Higher doses of ESA were associated with inflammation and a higher risk of MACE.
Keywords: ESA; anaemia; chronic kidney disease; dialysis; epidemiology; haemoglobin; inflammation; iron.
© The Author(s) 2020. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Kidney Disease: Improving Global Outcomes CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013; 3: 1–150 - PubMed
-
- Collins AJ. Influence of target hemoglobin in dialysis patients on morbidity and mortality. Kidney Int Suppl 2002; 80: 44–48 - PubMed
-
- Ofsthun N, Labrecque J, Lacson E. et al. The effects of higher hemoglobin levels on mortality and hospitalization in hemodialysis patients. Kidney Int 2003; 63: 1908–1914 - PubMed
-
- Rigatto C, Parfrey P, Foley R. et al. Congestive heart failure in renal transplant recipients: risk factors, outcomes, and relationship with ischemic heart disease. J Am Soc Nephrol 2002; 13: 1084–1090 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
