

Comprehensive analysis of genetic and clinical characteristics of 30 patients with X-linked juvenile retinoschisis in China
- PMID: 33124204
- PMCID: PMC8359357
- DOI: 10.1111/aos.14642
Comprehensive analysis of genetic and clinical characteristics of 30 patients with X-linked juvenile retinoschisis in China
Abstract
Purpose: To provides the clinical and genetic characteristics of a series of Chinese patients with X-linked juvenile retinoschisis (XLRS) through multimodal imaging and next-generation sequencing.
Methods: Thirty patients (60 eyes) from 29 unrelated families of Chinese origin with XLRS were screened using multigene panel testing, and underwent a complete clinical evaluation. All variants identified in this study and reported in the Human Gene Mutation Database were analysed.
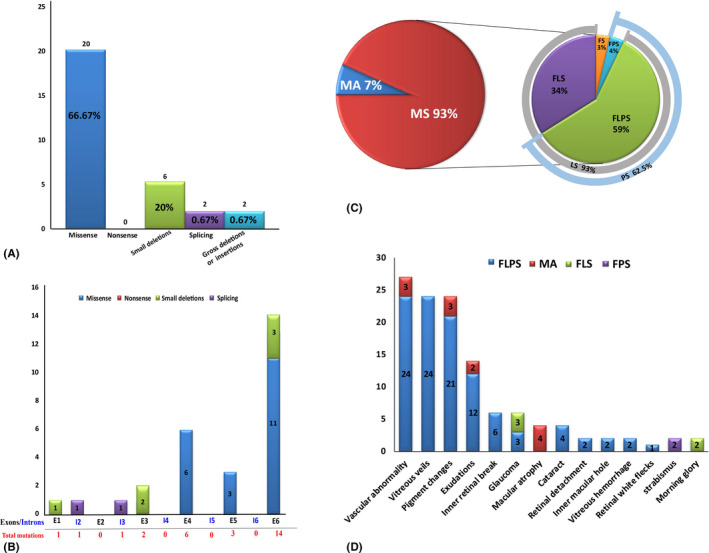
Results: Twenty-five distinct variants in the retinoschisin gene were identified, of which eight were novel, and one was de novo. Missense mutations were the most prevalent type, and mutation hot spot was localized in the discoidin domain. The mean Snellen best-corrected visual acuity was 0.28 ± 0.17. Of all eyes presenting with schisis, 92.86% had lamellar schisis and 62.5% had peripheral schisis. Schisis changes mostly involved inner and outer nuclear layers. X-linked juvenile retinoschisis (XLRS) patients had a high incidence of complications, and peripheral schisis was a risk factor for it. No obvious genotype-phenotype association was observed.
Conclusion: This study provides comprehensive analyses of the genetic and clinical characteristics of XLRS in a cohort of Chinese patients. The fourth de novo mutation in RS1 was identified. And we show that XLRS has a wide spectrum of clinical characteristics; hence, molecular diagnosis is crucial for its diagnosis, differential diagnosis and genetic counselling. Peripheral schisis is a risk factor for the high incidence of complications, and no clear genotype-phenotype correlations were found.
Keywords: RS1; Chinese population; X-linked retinoschisis; clinical diagnosis; molecular genetics; optical coherence tomography.
© 2020 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Figures
References
-
- AA (1998): Functional implications of the spectrum of mutations found in 234 cases with X‐linked juvenile retinoschisis. The Retinoschisis Consortium. Human Mol Genet 7: 1185–1192. - PubMed
-
- Ambler JS & Gutman FA (1991): Retinal detachment and retinoschisis. Ophthalmology 98: 1. - PubMed
-
- Ando A, Takahashi K, Sho K, Matsushima M, Okamura A & Uyama M (2000): Histopathological findings of X‐linked retinoschisis with neovascular glaucoma. Graefes Arch Clin Exp 238: 1–7. - PubMed
-
- Campbell JP, Skalet AH & Lauer AK (2015): Vitreous veils associated with congenital X‐linked retinoschisis. JAMA Ophthalmol 133: e151155. - PubMed
MeSH terms
Substances
Grants and funding
- 2017ZZ01020/Shanghai clinical medical center of ocular disease
- NSFC81770925/the National Natural Science Foundation of China
- NSFC81790641/the National Natural Science Foundation of China
- 2018PT32019/the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences
- XHLHGG201807/Xuhui district health and family planning commission key disease joint project
LinkOut - more resources
Full Text Sources
