

Review
doi: 10.4269/ajtmh.20-0712.
Case Report: Sparganosis of the Cauda Equina
Affiliations
- PMID: 33124542
- PMCID: PMC7790082
- DOI: 10.4269/ajtmh.20-0712
Item in Clipboard
Review
Case Report: Sparganosis of the Cauda Equina
Am J Trop Med Hyg.
2021 Jan.
Abstract
Spinal sparganosis of the cauda equina has been rarely reported. A 54-year-old man presented at the hospital after having experienced lower back pain for 10 months, progressive weakness and numbness of the left leg for 4 months, and urinary incontinence for 3 weeks. Magnetic resonance imaging of the lumbosacral spine revealed a heterogeneous enhancing mass at the T12-S1 level. Spinal sparganosis was diagnosed by histological examination and molecular identification of the parasite in the tissue section. The patient was treated with a high dose of praziquantel because the parasitic mass was only partially removed and symptoms worsened following surgery.
Figures
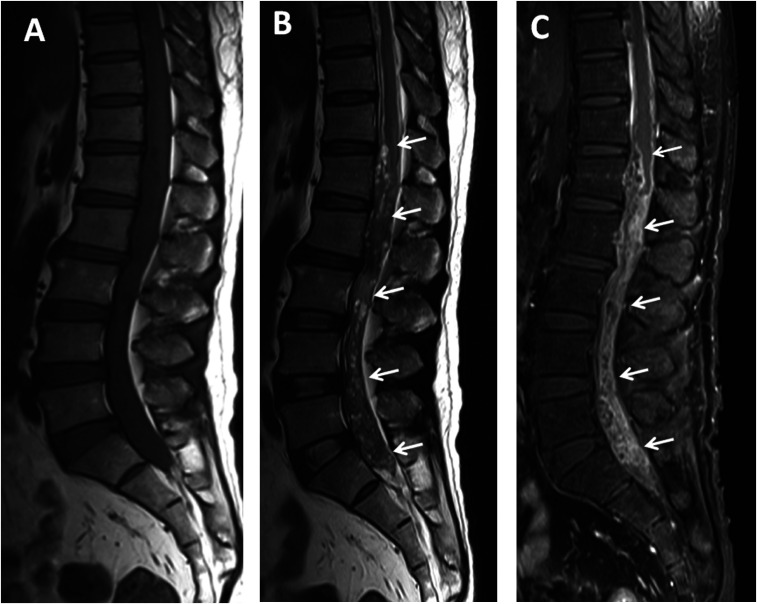
Magnetic resonance imaging lumbosacral spines, sagittal plane: T1WI (A), T2WI (B), and gadolinium (GD)-enhanced T1WI with fat suppression (C) showed a long mass-like lesion at the T12-S1 level (arrows). The lesion exhibited isosignal intensity at T1WI, mixed hypo/hypersignal intensity at T2WI, and heterogeneous and irregular enhancement at T1FS with GD. Hypersignal intensity of the spinal cord above the lesion was also detected in the T2WI image (B), which represented diffuse spinal cord edema.
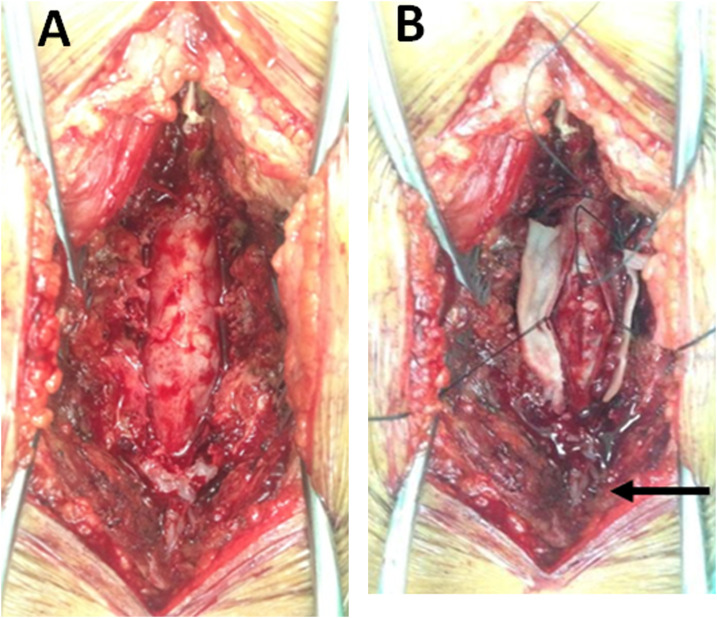
Operative field pictures: surgical exposure of the spinal cord, (A) before opening the dura mater, and (B) after opening the dura mater showed enlargement of the thecal sac (A) and a matted lesion with small cysts (arrow) in the subarachnoid space (B). This figure appears in color at www.ajtmh.org .
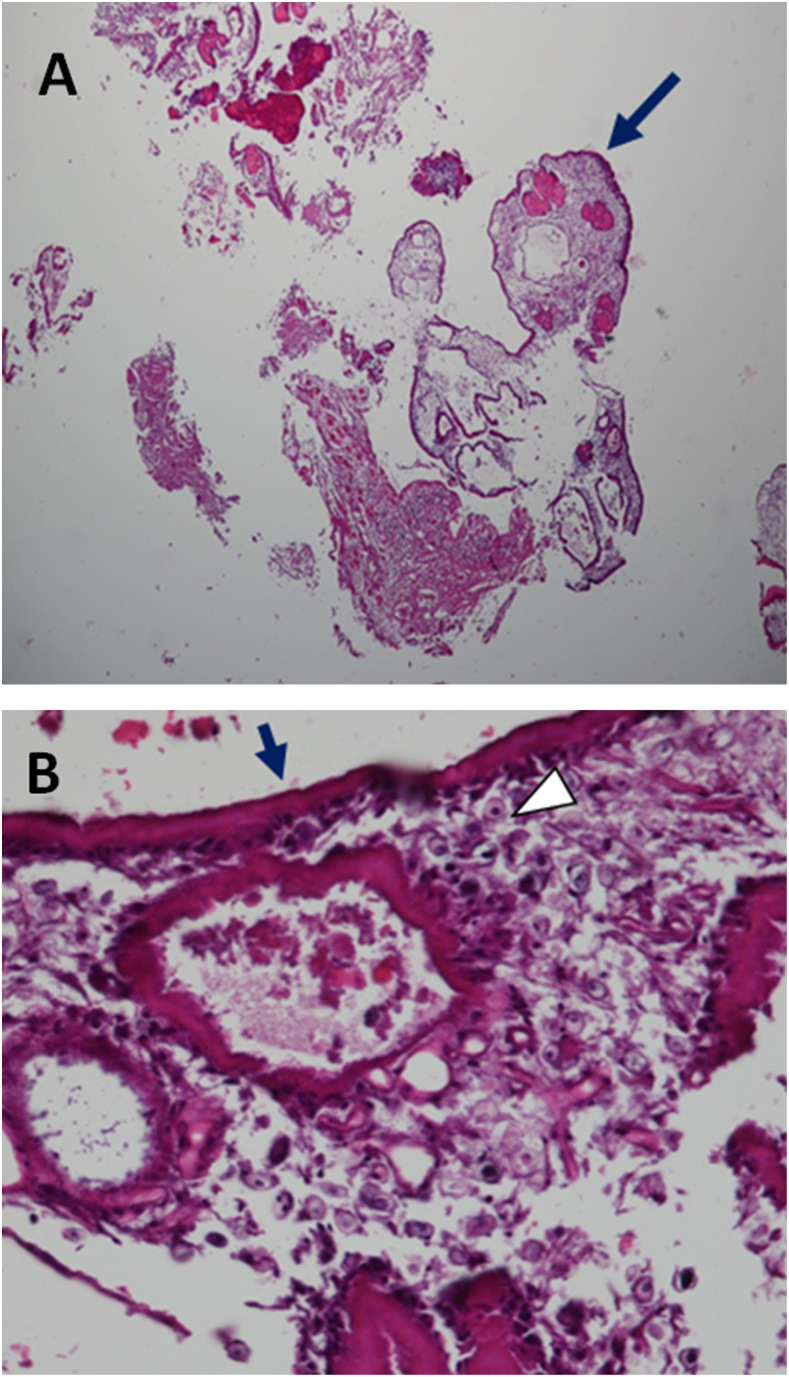
Hematoxylin and eosin–stained section: (A) a photograph at ×40 magnification and (B) at ×400 magnification revealed cross sections of a parasitic organism surrounded by degenerative connective tissues without specific inflammatory reaction (A, arrow), with a thick eosinophilic tegumental structure (B, arrow). The subtegumental layer showed several calcareous corpuscles in a loose parenchyma (B, arrowhead). This figure appears in color at www.ajtmh.org .
References
-
- Anantaphruti MT, Nawa Y, Vanvanitchai Y, 2011. Human sparganosis in Thailand: an overview. Acta Trop 118: 171–176. - PubMed
-
- Kwon JH, Kim JS, 2004. Sparganosis presenting as a conus medullaris lesion: case report and literature review of the spinal sparganosis. Arch Neurol 61: 1126–1128. - PubMed
-
- Chung SW, Kim YH, Lee EJ, Kim DH, Kim GY, 2012. Two cases of pulmonary and pleural sparganosis confirmed by tissue biopsy and immunoserology. Braz J Infect Dis 16: 200–203. - PubMed
-
- Kim DG, Paek SH, Chang KH, Wang KC, Jung HW, Kim HJ, Chi JG, Choi KS, Han DH, 1996. Cerebral sparganosis: clinical manifestations, treatment, and outcome. J Neurosurg 85: 1066–1071. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
