

Acute kidney injury associated with COVID-19: A retrospective cohort study
- PMID: 33125416
- PMCID: PMC7598516
- DOI: 10.1371/journal.pmed.1003406
Acute kidney injury associated with COVID-19: A retrospective cohort study
Abstract
Background: Initial reports indicate a high incidence of acute kidney injury (AKI) in Coronavirus Disease 2019 (COVID-19), but more data are required to clarify if COVID-19 is an independent risk factor for AKI and how COVID-19-associated AKI may differ from AKI due to other causes. We therefore sought to study the relationship between COVID-19, AKI, and outcomes in a retrospective cohort of patients admitted to 2 acute hospitals in Derby, United Kingdom.
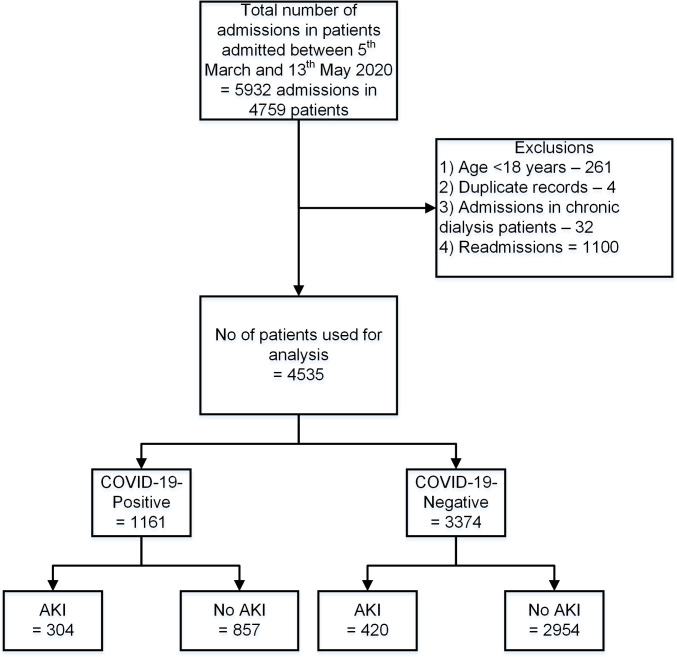
Methods and findings: We extracted electronic data from 4,759 hospitalised patients who were tested for COVID-19 between 5 March 2020 and 12 May 2020. The data were linked to electronic patient records and laboratory information management systems. The primary outcome was AKI, and secondary outcomes included in-hospital mortality, need for ventilatory support, intensive care unit (ICU) admission, and length of stay. As compared to the COVID-19-negative group (n = 3,374), COVID-19 patients (n = 1,161) were older (72.1 ± 16.1 versus 65.3 ± 20.4 years, p < 0.001), had a greater proportion of men (56.6% versus 44.9%, p < 0.001), greater proportion of Asian ethnicity (8.3% versus 4.0%, p < 0.001), and lower proportion of white ethnicity (75.5% versus 82.5%, p < 0.001). AKI developed in 304 (26.2%) COVID-19-positive patients (COVID-19 AKI) and 420 (12.4%) COVID-19-negative patients (AKI controls). COVID-19 patients aged 65 to 84 years (odds ratio [OR] 1.67, 95% confidence interval [CI] 1.11 to 2.50), needing mechanical ventilation (OR 8.74, 95% CI 5.27 to 14.77), having congestive cardiac failure (OR 1.72, 95% CI 1.18 to 2.50), chronic liver disease (OR 3.43, 95% CI 1.17 to 10.00), and chronic kidney disease (CKD) (OR 2.81, 95% CI 1.97 to 4.01) had higher odds for developing AKI. Mortality was higher in COVID-19 AKI versus COVID-19 patients without AKI (60.5% versus 27.4%, p < 0.001), and AKI was an independent predictor of mortality (OR 3.27, 95% CI 2.39 to 4.48). Compared with AKI controls, COVID-19 AKI was observed in a higher proportion of men (58.9% versus 51%, p = 0.04) and lower proportion with white ethnicity (74.7% versus 86.9%, p = 0.003); was more frequently associated with cerebrovascular disease (11.8% versus 6.0%, p = 0.006), chronic lung disease (28.0% versus 19.3%, p = 0.007), diabetes (24.7% versus 17.9%, p = 0.03), and CKD (34.2% versus 20.0%, p < 0.001); and was more likely to be hospital acquired (61.2% versus 46.4%, p < 0.001). Mortality was higher in the COVID-19 AKI as compared to the control AKI group (60.5% versus 27.6%, p < 0.001). In multivariable analysis, AKI patients aged 65 to 84 years, (OR 3.08, 95% CI 1.77 to 5.35) and ≥85 years of age (OR 3.54, 95% CI 1.87 to 6.70), peak AKI stage 2 (OR 1.74, 95% CI 1.05 to 2.90), AKI stage 3 (OR 2.01, 95% CI 1.13 to 3.57), and COVID-19 (OR 3.80, 95% CI 2.62 to 5.51) had higher odds of death. Limitations of the study include retrospective design, lack of urinalysis data, and low ethnic diversity of the region.
Conclusions: We observed a high incidence of AKI in patients with COVID-19 that was associated with a 3-fold higher odds of death than COVID-19 without AKI and a 4-fold higher odds of death than AKI due to other causes. These data indicate that patients with COVID-19 should be monitored for the development of AKI and measures taken to prevent this.
Trial registration: ClinicalTrials.gov NCT04407156.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: MWT is a member of the Editorial Board of PLOS Medicine NVK, RJF & NMS have declared that no competing interests exist.
Figures
References
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
