

Laboratory Findings Associated With Severe Illness and Mortality Among Hospitalized Individuals With Coronavirus Disease 2019 in Eastern Massachusetts
- PMID: 33125498
- PMCID: PMC7599467
- DOI: 10.1001/jamanetworkopen.2020.23934
Laboratory Findings Associated With Severe Illness and Mortality Among Hospitalized Individuals With Coronavirus Disease 2019 in Eastern Massachusetts
Abstract
Importance: The coronavirus disease 2019 (COVID-19) pandemic has placed unprecedented stress on health systems across the world, and reliable estimates of risk for adverse hospital outcomes are needed.
Objective: To quantify admission laboratory and comorbidity features associated with critical illness and mortality risk across 6 Eastern Massachusetts hospitals.
Design, setting, and participants: Retrospective cohort study of all individuals admitted to the hospital who tested positive for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) by polymerase chain reaction across these 6 hospitals through June 5, 2020, using hospital course, prior diagnoses, and laboratory values in emergency department and inpatient settings from 2 academic medical centers and 4 community hospitals. The data were extracted on June 11, 2020, and the analysis was conducted from June to July 2020.
Exposures: SARS-CoV-2.
Main outcomes and measures: Severe illness defined by admission to intensive care unit, mechanical ventilation, or death.
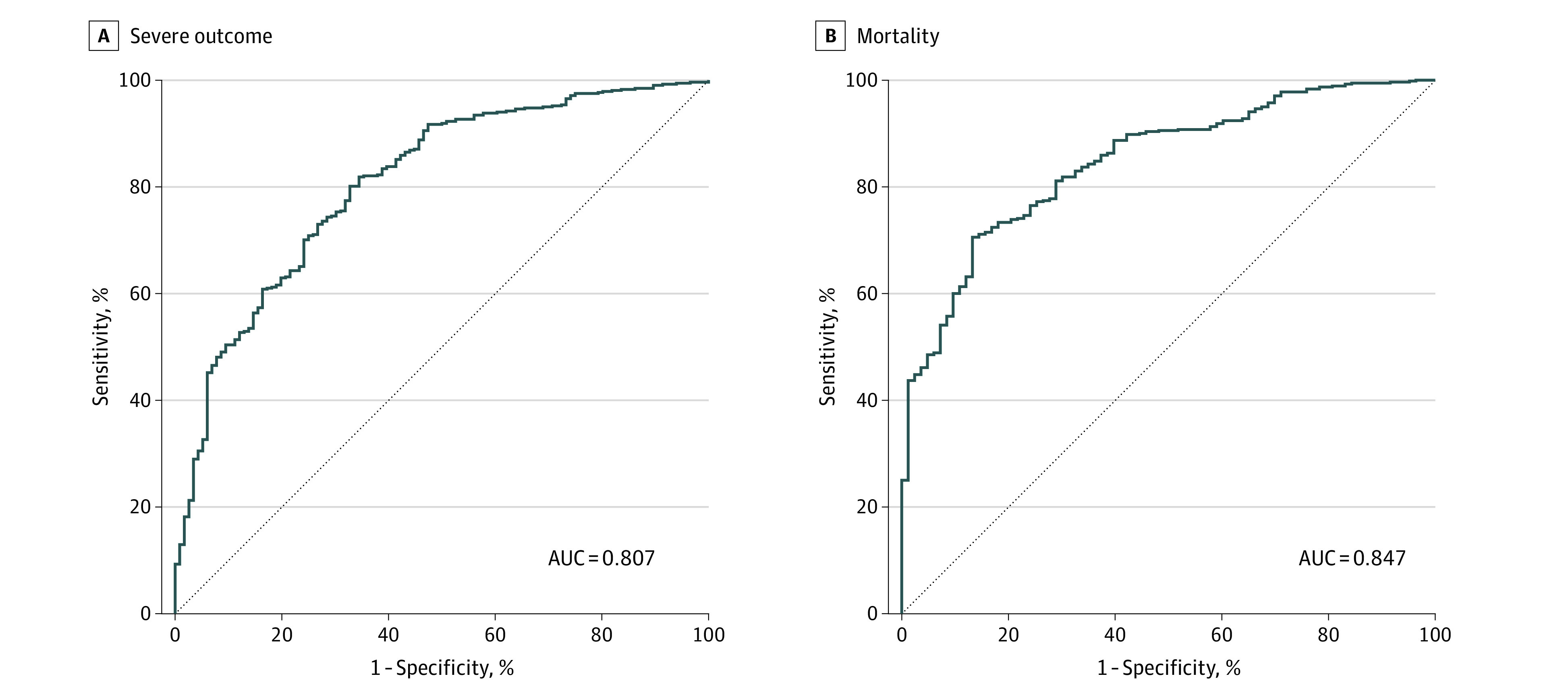
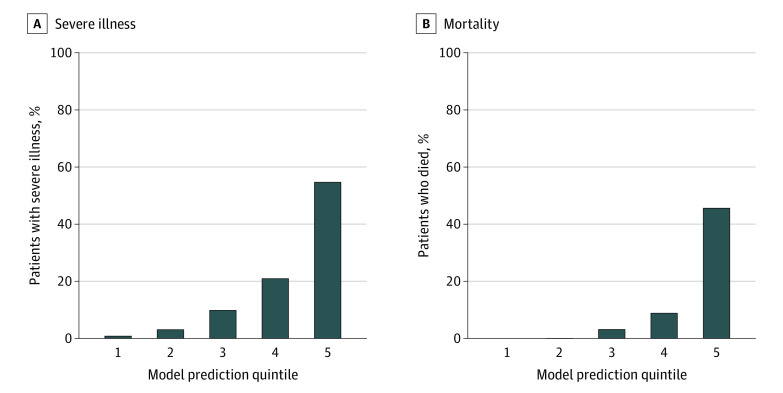
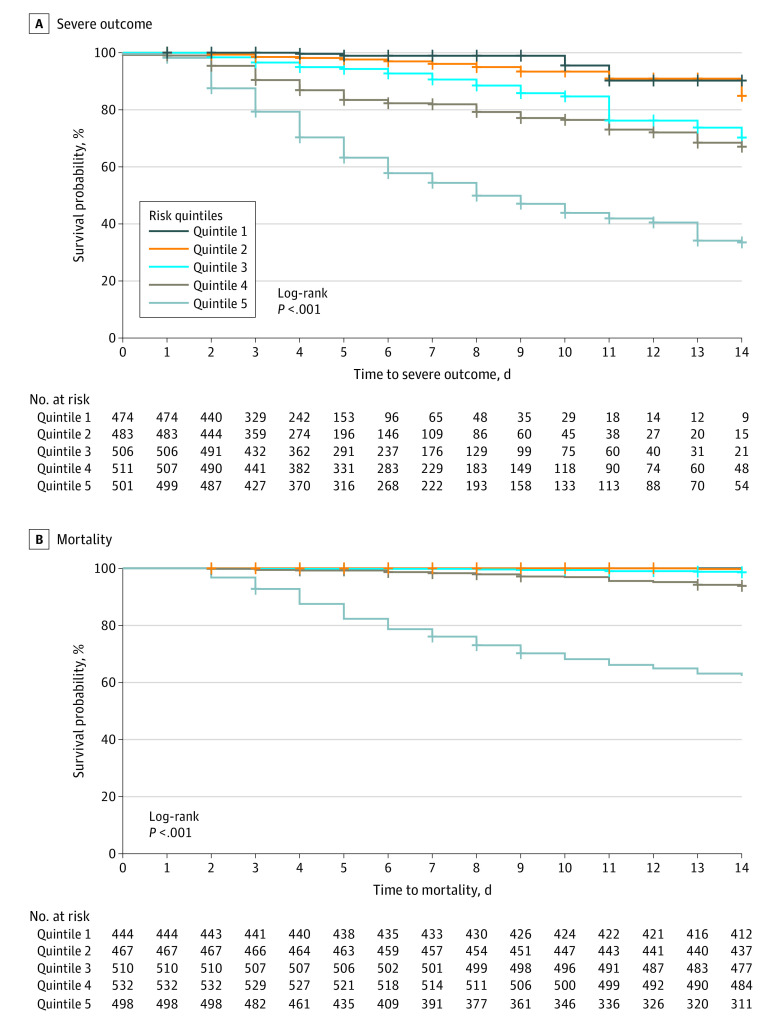
Results: Of 2511 hospitalized individuals who tested positive for SARS-CoV-2 (of whom 50.9% were male, 53.9% White, and 27.0% Hispanic, with a mean [SD ]age of 62.6 [19.0] years), 215 (8.6%) were admitted to the intensive care unit, 164 (6.5%) required mechanical ventilation, and 292 (11.6%) died. L1-regression models developed in 3 of these hospitals yielded an area under the receiver operating characteristic curve of 0.807 for severe illness and 0.847 for mortality in the 3 held-out hospitals. In total, 212 of 292 deaths (72.6%) occurred in the highest-risk mortality quintile.
Conclusions and relevance: In this cohort, specific admission laboratory studies in concert with sociodemographic features and prior diagnosis facilitated risk stratification among individuals hospitalized for COVID-19.
Conflict of interest statement
Figures
Update of
-
Laboratory findings associated with severe illness and mortality among hospitalized individuals with coronavirus disease 2019 in Eastern Massachusetts.medRxiv [Preprint]. 2020 Aug 28:2020.05.04.20090555. doi: 10.1101/2020.05.04.20090555. medRxiv. 2020. Update in: JAMA Netw Open. 2020 Oct 1;3(10):e2023934. doi: 10.1001/jamanetworkopen.2020.23934. PMID: 32869044 Free PMC article. Updated. Preprint.
References
-
- Richardson S, Hirsch JS, Narasimhan M, et al. ; the Northwell COVID-19 Research Consortium . Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052-2059. doi:10.1001/jama.2020.6775 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
