

Susac syndrome (Retino-cochleo-cerebral vasculitis), the ophthalmologist in the role of the whistleblower
- PMID: 33125601
- PMCID: PMC7599291
- DOI: 10.1186/s12348-020-00217-z
Susac syndrome (Retino-cochleo-cerebral vasculitis), the ophthalmologist in the role of the whistleblower
Abstract
Background/purpose: Susac syndrome is a rare microangiopathy of suspected autoimmune origin affecting arteries of the retina, the cochlea and the brain. The aim of the study was to give a review of the disease entity and determine the proportion of cases and their characteristics in a uveitis referral centre.
Patients and methods: Charts of patients with the diagnosis of Susac syndrome seen in the Uveitis Clinic of the Centre for Ophthalmic Specialised Care (COS), Lausanne, Switzerland were reviewed retrospectively to determine the frequency of such cases in a uveitis referral centre. Clinical symptoms and signs, functional data, imaging signs and evolution were analysed in the 3 COS cases and one case shared with the Uveitis Clinic of the Department of Ophthalmology, University of Innsbruck, Austria. Characteristic signs were searched possibly allowing a prompt diagnosis.
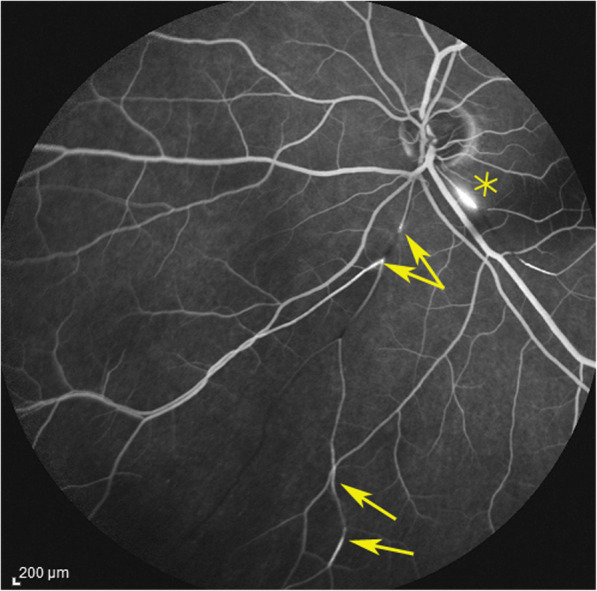
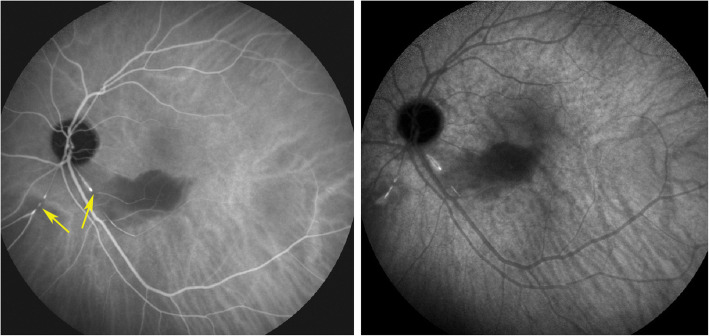
Results: During the period from 1994 to 2019 (24 years, 2045 patients), 3 charts with the diagnosis of Susac syndrome were found (0.15%). The whole collective, including the additional case, comprised three women aged 28, 32 and 63 at presentation and one man, aged 42. None of the 3 cases that were referred were diagnosed beforehand. The characteristic item found in all 4 cases was the abrupt arterial stop or segmental interruption of arteries and increased staining of arterial wall on angiography more clearly shown on indocyanine green angiography that can potentially be proposed as a crucial diagnostic element. All 4 cases responded to dual steroidal and non-steroidal immunosuppression. Under treatment, all four patients did not show any further evolution.
Conclusion: Susac syndrome is a multilocation arteritis of the head that can involve the eye, ear and brain often first diagnosed by the ophthalmologist. The diagnosis is rapidly reached in uveitis referral centres but seems to be missed otherwise, A helpful angiographic sign to be searched is an abrupt or segmental arterial stop and increased staining of the arterial wall more clearly seen on indocyanine green angiography. Patients often present first to the ophthalmologist who should be acting as a whistleblower to avoid severe involvement of the brain.
Keywords: Branch retinal artery occlusion (BRAO); Fluorescein angiography; Indocyanine green angiography; Susac syndrome.
Conflict of interest statement
There is no financial disclosure.
Figures









References
Publication types
LinkOut - more resources
Full Text Sources
