

Correlations between weight-bearing 3D bone architecture and dynamic plantar pressure measurements in the diabetic foot
- PMID: 33126903
- PMCID: PMC7597032
- DOI: 10.1186/s13047-020-00431-x
Correlations between weight-bearing 3D bone architecture and dynamic plantar pressure measurements in the diabetic foot
Abstract
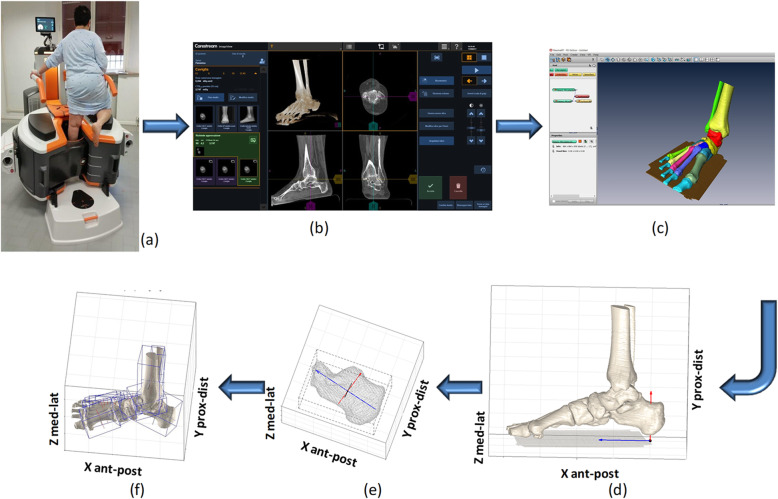
Background: Measurements of plantar loading reveal foot-to-floor interaction during activity, but information on bone architecture cannot be derived. Recently, cone-beam computer tomography (CBCT) has given visual access to skeletal structures in weight-bearing. The combination of the two measures has the potential to improve clinical understanding and prevention of diabetic foot ulcers. This study explores the correlations between static 3D bone alignment and dynamic plantar loading.
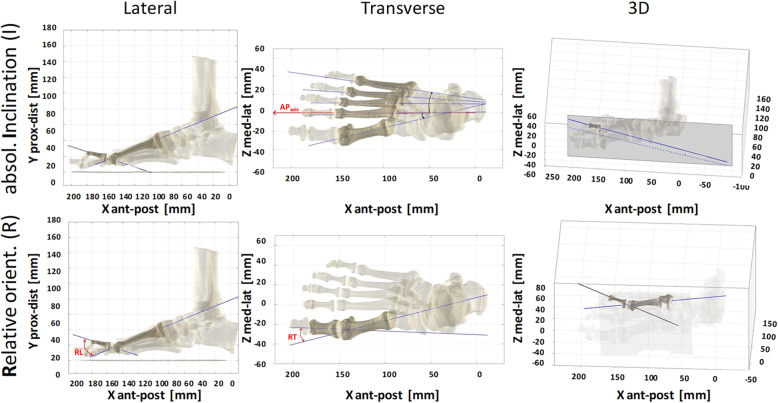
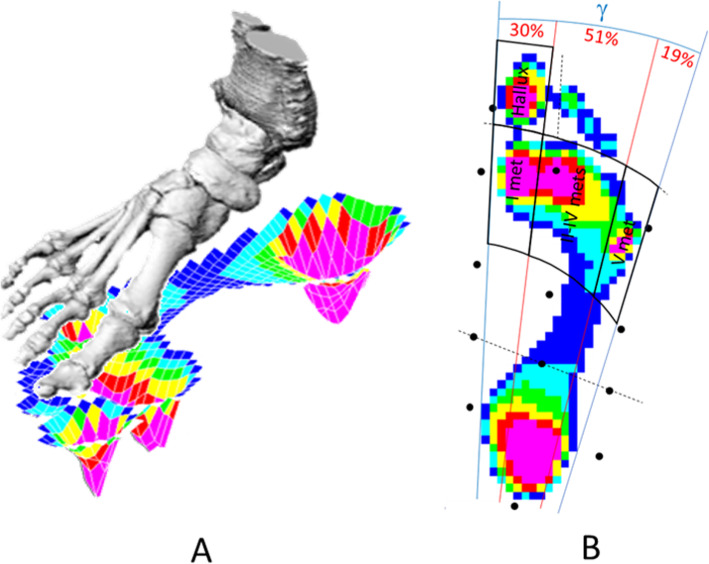
Methods: Sixteen patients with diabetes were enrolled (group ALL): 15 type 1 with (N, 7) and without (D, 8) diabetic neuropathy, and 1 with latent autoimmune diabetes. CBCT foot scans were taken in single-leg upright posture. 3D bone models were obtained by image segmentation and aligned in a foot anatomical reference frame. Absolute inclination and relative orientation angles and heights of the bones were calculated. Pressure patterns were also acquired during barefoot level walking at self-selected speed, from which regional peak pressure and absolute and normalised pressure-time integral were worked out at hallux and at first, central and fifth metatarsals (LOAD variables) as averaged over five trials. Correlations with 3D alignments were searched also with arch index, contact time, age, BMI, years of disease and a neuropathy-related variable.
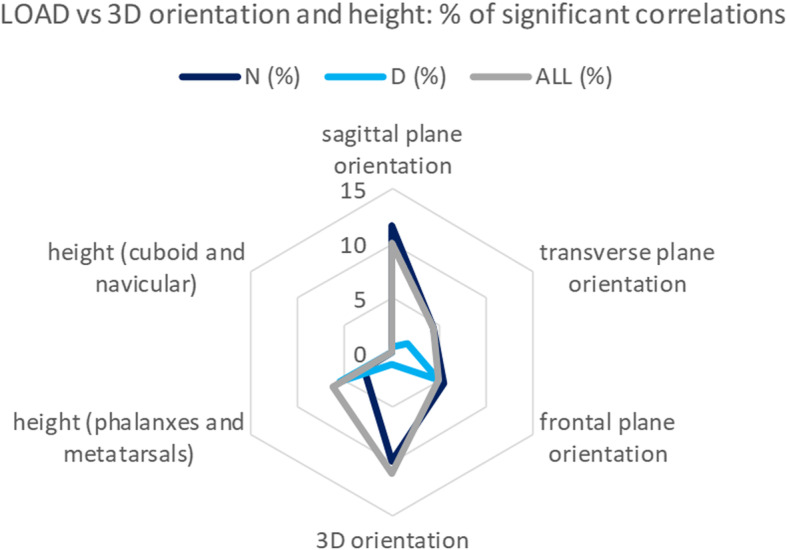
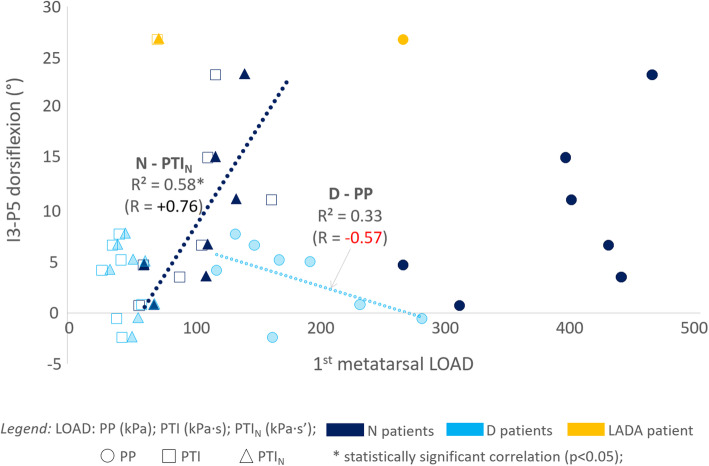
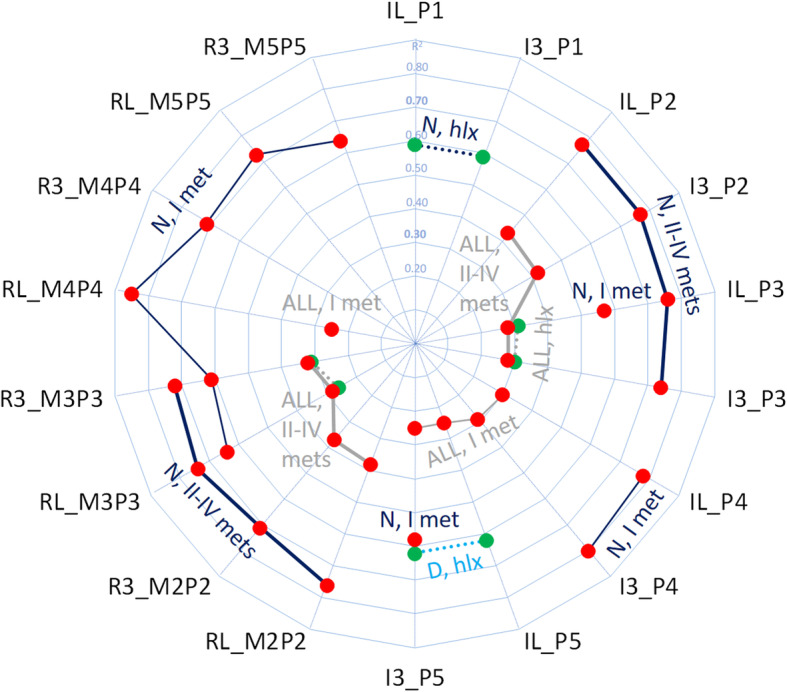
Results: Lateral and 3D angles showed the highest percentage of significant (p < 0.05) correlations with LOAD. These were weak-to-moderate in the ALL group, moderate-to-strong in N and D. LOAD under the central metatarsals showed moderate-to-strong correlation with plantarflexion of the 2nd and 3rd phalanxes in ALL and N. LOAD at the hallux increased with plantarflexion at the 3rd phalanx in ALL, at 1st phalanx in N and at 5th phalanx in D. Arch index correlated with 1st phalanx plantarflexion in ALL and D; contact time showed strong correlation with 2nd and 3rd metatarsals and with 4th phalanx dorsiflexion in D.
Conclusion: These preliminary original measures reveal that alteration of plantar dynamic loading patterns can be accounted for peculiar structural changes of foot bones. Load under the central metatarsal heads were correlated more with inclination of the corresponding phalanxes than metatarsals. Further analyses shall detect to which extent variables play a role in the many group-specific correlations.
Keywords: Bone positions and orientations; Cone-beam weight-bearing computed tomography; Diabetic foot; Dynamic plantar loading; Foot bone models; Principal component analysis.
Conflict of interest statement
All authors declare that there are no personal or commercial relationships related to this work that would lead to a conflict of interest.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
