

Contemporary Risk of Surgery in Patients With Ulcerative Colitis and Crohn's Disease: A Meta-Analysis of Population-Based Cohorts
- PMID: 33127595
- PMCID: PMC8934200
- DOI: 10.1016/j.cgh.2020.10.039
Contemporary Risk of Surgery in Patients With Ulcerative Colitis and Crohn's Disease: A Meta-Analysis of Population-Based Cohorts
Abstract
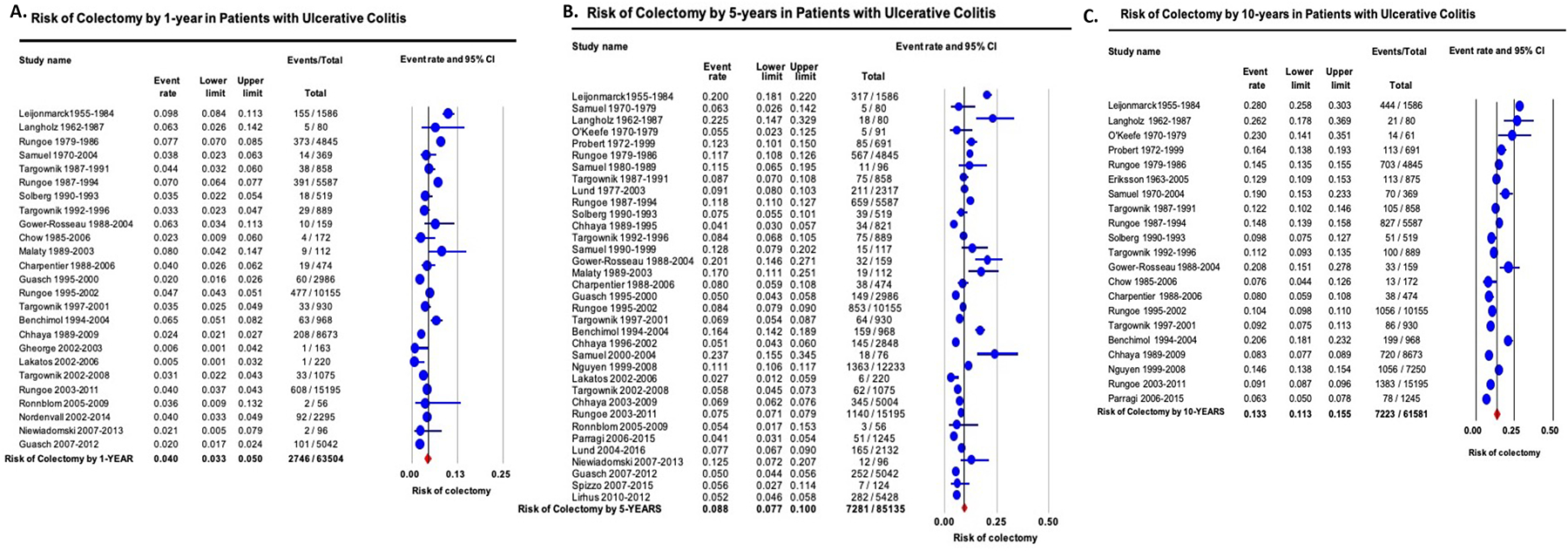
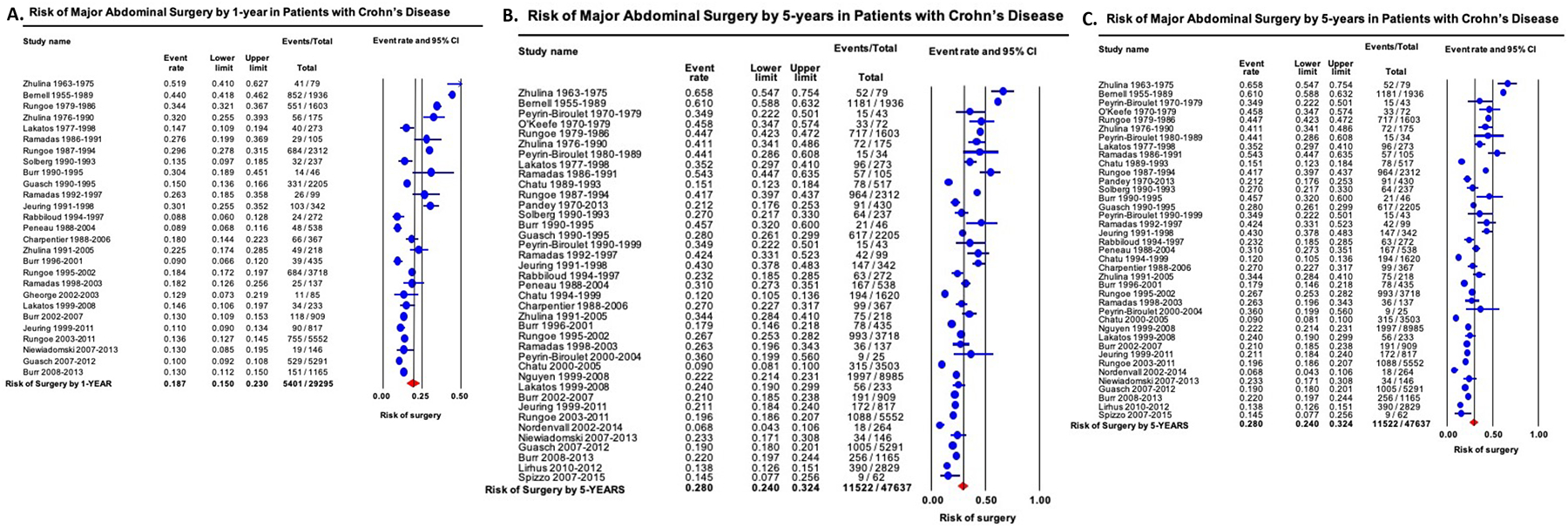
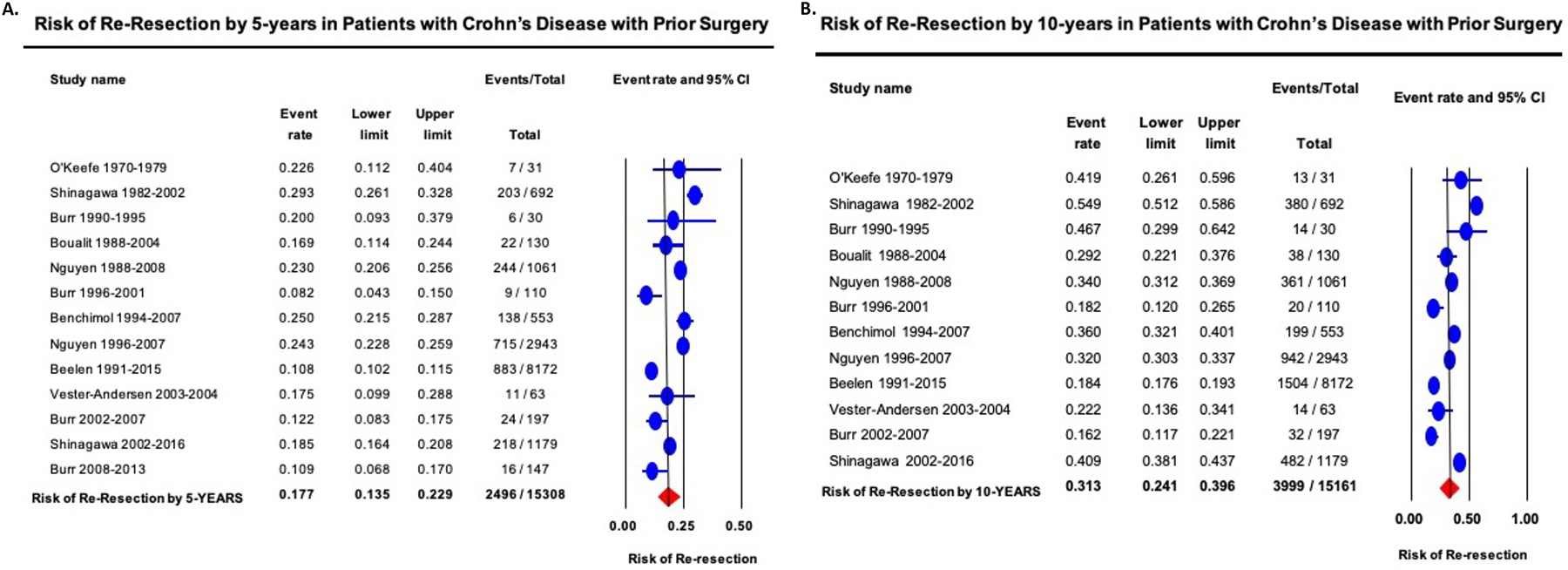
Background & aims: We conducted a systematic review with meta-analysis to estimate rates and trends of colectomy in patients with ulcerative colitis (UC), and of primary and re-resection in patients with Crohn's disease (CD), focusing on contemporary risks.
Methods: Through a systematic review until September 3, 2019, we identified population-based cohort studies that reported patient-level cumulative risk of surgery in patients with UC and CD. We evaluated overall and contemporary risk (after 2000) of surgery and analyzed time trends through mixed-effects meta-regression.
Results: In patients with UC (26 studies), the overall 1-, 5-, and 10-year risks of colectomy was 4.0% (95% CI, 3.3-5.0), 8.8% (95% CI, 7.7-10.0), and 13.3% (95% CI, 11.3-15.5), respectively, with a decrease in risk over time (P < .001). Corresponding contemporary risks were 2.8% (95% CI, 2.0-3.9), 7.0% (95% CI, 5.7-8.6), and 9.6% (95% CI, 6.3-14.2), respectively. In patients with CD (22 studies), the overall 1-, 5-, and 10-year risk of surgery was 18.7% (95% CI, 15.0-23.0), 28.0% (95% CI, 24.0-32.4), and 39.5% (95% CI, 33.3-46.2), respectively, with a decrease in risk over time (P < .001). Corresponding contemporary risks were 12.3% (95% CI, 10.8-14.0), 18.0% (95% CI, 15.4-21.0), and 26.2% (95% CI, 23.4-29.4), respectively. In a meta-analysis of 8 studies in patients with CD with prior resection, the cumulative risk of a second resection at 5 and 10 years after the first resection was 17.7% (95% CI, 13.5-22.9) and 31.3% (95% CI, 24.1-39.6), respectively.
Conclusions: Patient-level risks of surgery have decreased significantly over time, with a 5-year cumulative risk of surgery of 7.0% in UC and 18.0% in CD in contemporary cohorts. This decrease may be related to early detection and/or better treatment.
Keywords: Disease Modification; Inflammatory Bowel Diseases; Natural History; Resection; Tumor Necrosis Factor.
Copyright © 2021. Published by Elsevier Inc.
Figures
Comment in
-
Lower Surgical Risks in "Contemporary" IBD Cohorts: A Reflection of Better Quality of Care or Statistics?Clin Gastroenterol Hepatol. 2021 Oct;19(10):2029-2030. doi: 10.1016/j.cgh.2021.01.047. Epub 2021 Jan 29. Clin Gastroenterol Hepatol. 2021. PMID: 33524597 No abstract available.
-
A Patient Perspective on Contemporary Risk of Surgery in Patients With Ulcerative Colitis and Crohn's Disease.Clin Gastroenterol Hepatol. 2022 Feb;20(2):469-470. doi: 10.1016/j.cgh.2021.04.012. Epub 2021 Apr 9. Clin Gastroenterol Hepatol. 2022. PMID: 33839280 No abstract available.
References
-
- Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 2018;390:2769–2778. - PubMed
-
- Coward S, Clement F, Benchimol EI, et al. Past and Future Burden of Inflammatory Bowel Diseases Based on Modeling of Population-Based Data. Gastroenterology 2019;156:1345–1353.e4. - PubMed
-
- King JA, Underwood FE, Panaccione N, et al. Trends in hospitalisation rates for inflammatory bowel disease in western versus newly industrialised countries: a population-based study of countries in the Organisation for Economic Co-operation and Development. The Lancet Gastroenterology & Hepatology 2019;4:287–295. - PubMed
-
- Frolkis AD, Dykeman J, Negron ME, et al. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology 2013;145:996–1006. - PubMed
