

DECAF score as a mortality predictor for acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis
- PMID: 33127631
- PMCID: PMC7604856
- DOI: 10.1136/bmjopen-2020-037923
DECAF score as a mortality predictor for acute exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis
Abstract
Objectives: This study was conducted to assess the association between the Dyspnea, Eosinopenia, Consolidation, Acidemia and Atrial Fibrillation (DECAF) scores and the prognosis of patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD), to evaluate the specific predictive and prognostic value of DECAF scores and to explore the effectiveness of different cut-off values in risk stratification of patients with AECOPD.
Design: Systematic review and meta-analysis.
Participants: Adult patients diagnosed with AECOPD (over 18 years of age).
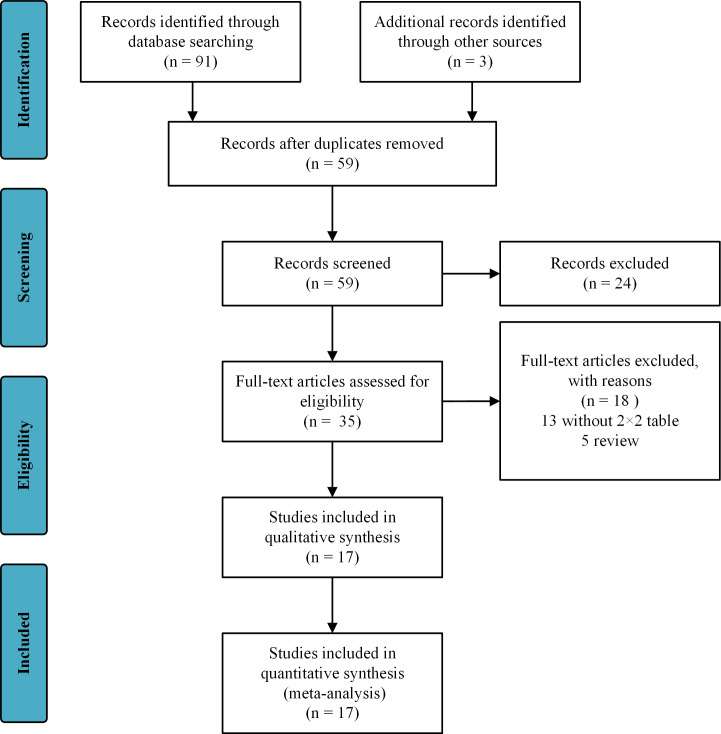
Primary and secondary outcome measures: Electronic databases, including the Cochrane Library, PubMed, the Embase and the WOS, and the reference lists in related articles were searched for studies published up to September 2019. The identified studies reported the prognostic value of DECAF scores in patients with AECOPD.
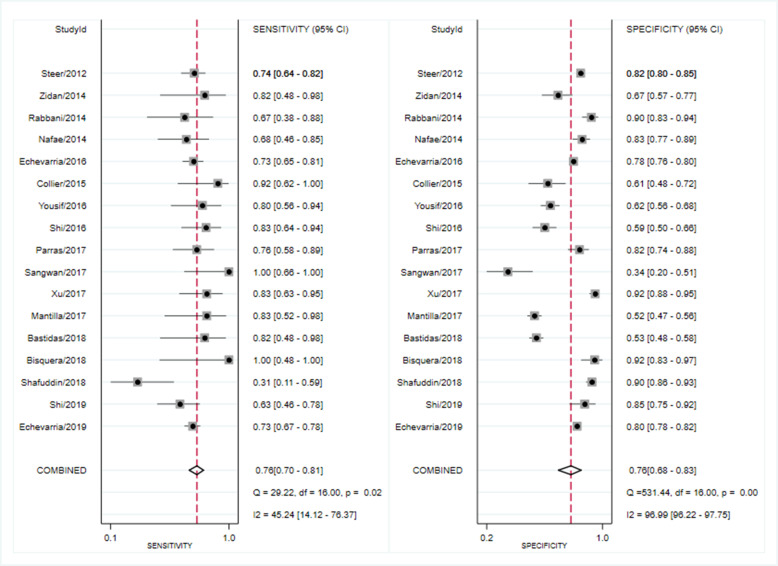
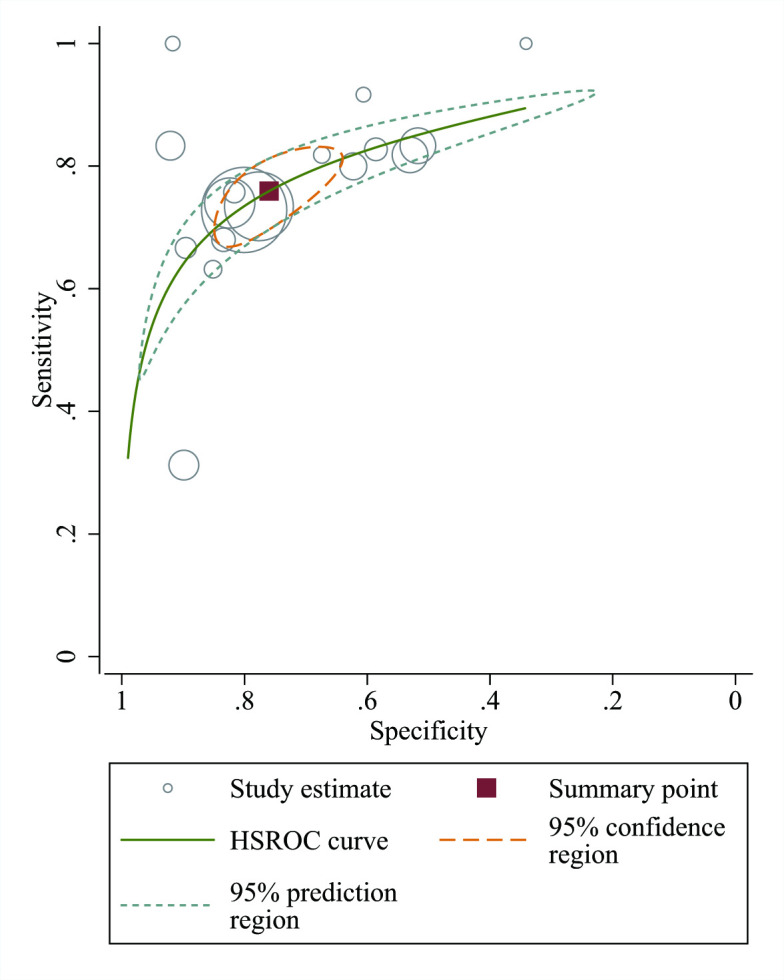
Results: Seventeen studies involving 8329 participants were included in the study. Quantitative analysis demonstrated that elevated DECAF scores were associated with high mortality risk (weighted mean difference=1.87; 95% CI 1.19 to 2.56). In the accuracy analysis, DECAF scores showed good prognostic accuracy for both in-hospital and 30-day mortality (area under the receiver operating characteristic curve: 0.83 (0.79-0.86) and 0.79 (0.76-0.83), respectively). When the prognostic value was compared with that of other scoring systems, DECAF scores showed better prognostic accuracy and stable clinical values than the modified DECAF; COPD and Asthma Physiology Score; BUN, Altered mental status, Pulse and age >65; Confusion, Urea, Respiratory Rate, Blood pressure and age >65; or Acute Physiology and Chronic Health Evaluation II scores.
Conclusion: The DECAF score is an effective and feasible predictor for short-term mortality. As a specific and easily scored predictor for patients with AECOPD, DECAF score is superior to other prognostic scores. The DECAF score can correctly identify most patients with AECOPD as low risk, and with the increase of cut-off value, the risk stratification of DECAF score in high-risk population increases significantly.
Keywords: adult intensive & critical care; chronic airways disease; respiratory medicine (see thoracic medicine).
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Procalcitonin (PCT) Improves the Accuracy and Sensitivity of Dyspnea, Eosinopenia, Consolidation, Acidemia and Atrial Fibrillation (DECAF) Score in Predicting AECOPD Patients Admission to ICU.Clin Lab. 2020 Mar 1;66(3). doi: 10.7754/Clin.Lab.2019.190612. Clin Lab. 2020. PMID: 32162862
-
Utility of the DECAF score for predicting survival of patients with COPD: a meta-analysis of diagnostic accuracy studies.Eur Rev Med Pharmacol Sci. 2021 Jun;25(11):4037-4050. doi: 10.26355/eurrev_202106_26045. Eur Rev Med Pharmacol Sci. 2021. PMID: 34156682
-
Comparative Analysis of the COPD Assessment Test and Modified DECAF Score in Predicting Clinical Outcomes Among Patients With Acute Exacerbation of COPD: A Prospective Observational Study.Cureus. 2025 Feb 25;17(2):e79605. doi: 10.7759/cureus.79605. eCollection 2025 Feb. Cureus. 2025. PMID: 40151756 Free PMC article.
-
Predictors of mortality in acute exacerbations of chronic obstructive pulmonary disease using the dyspnea, eosinopenia, consolidation, acidemia and atrial fibrillation score.Lung India. 2020 Jan-Feb;37(1):19-23. doi: 10.4103/lungindia.lungindia_114_19. Lung India. 2020. PMID: 31898616 Free PMC article.
-
A pooled analysis of the risk prediction models for mortality in acute exacerbation of chronic obstructive pulmonary disease.Clin Respir J. 2023 Aug;17(8):707-718. doi: 10.1111/crj.13606. Epub 2023 Mar 21. Clin Respir J. 2023. PMID: 36945821 Free PMC article. Review.
Cited by
-
Eosinopenia as a Prognostic Biomarker for Noninvasive Ventilation Use in COPD Exacerbations.J Pers Med. 2023 Apr 19;13(4):686. doi: 10.3390/jpm13040686. J Pers Med. 2023. PMID: 37109072 Free PMC article.
-
Prognostic Accuracy of DECAF and Ottawa COPD Risk Scores in Patients Presenting to the Emergency Department With COPD Exacerbation.J Acute Med. 2025 Mar 1;15(1):11-18. doi: 10.6705/j.jacme.202503_15(1).0002. J Acute Med. 2025. PMID: 40061304 Free PMC article.
-
Eosinophils and Chronic Respiratory Diseases in Hospitalized COVID-19 Patients.Front Immunol. 2021 Jun 2;12:668074. doi: 10.3389/fimmu.2021.668074. eCollection 2021. Front Immunol. 2021. PMID: 34149705 Free PMC article.
-
An International Validation of the "DECAF Score" to Predict Disease Severity and Hospital Mortality in Acute Exacerbation of COPD in the UAE.Hosp Pharm. 2024 Apr;59(2):234-240. doi: 10.1177/00185787231209218. Epub 2023 Nov 3. Hosp Pharm. 2024. PMID: 38450352 Free PMC article.
-
Factors Associated with Initial Treatment Failure in Inpatients with Exacerbation of Chronic Obstructive Pulmonary Disease: A Cohort Study.Int J Chron Obstruct Pulmon Dis. 2025 Jul 10;20:2349-2360. doi: 10.2147/COPD.S516855. eCollection 2025. Int J Chron Obstruct Pulmon Dis. 2025. PMID: 40661117 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials