

Plasma Proteomics Identify Biomarkers and Pathogenesis of COVID-19
- PMID: 33128875
- PMCID: PMC7574896
- DOI: 10.1016/j.immuni.2020.10.008
Plasma Proteomics Identify Biomarkers and Pathogenesis of COVID-19
Abstract
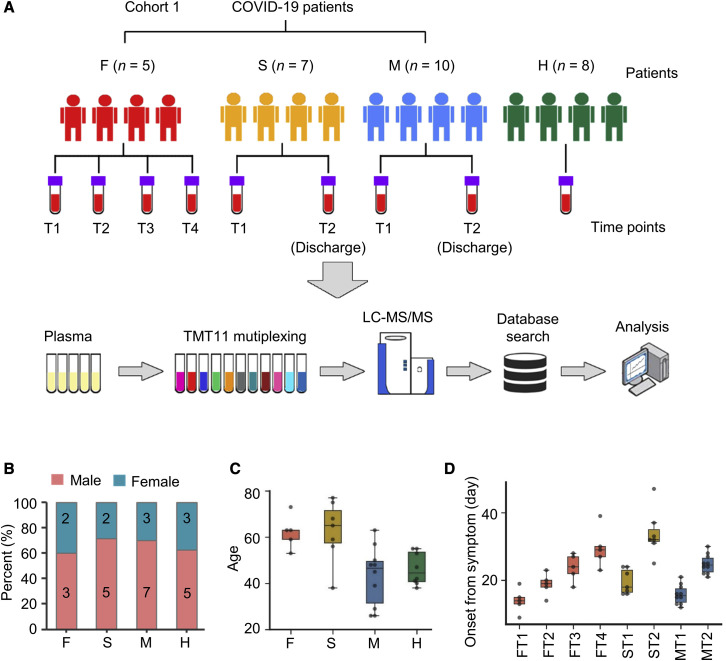
The coronavirus disease 2019 (COVID-19) pandemic is a global public health crisis. However, little is known about the pathogenesis and biomarkers of COVID-19. Here, we profiled host responses to COVID-19 by performing plasma proteomics of a cohort of COVID-19 patients, including non-survivors and survivors recovered from mild or severe symptoms, and uncovered numerous COVID-19-associated alterations of plasma proteins. We developed a machine-learning-based pipeline to identify 11 proteins as biomarkers and a set of biomarker combinations, which were validated by an independent cohort and accurately distinguished and predicted COVID-19 outcomes. Some of the biomarkers were further validated by enzyme-linked immunosorbent assay (ELISA) using a larger cohort. These markedly altered proteins, including the biomarkers, mediate pathophysiological pathways, such as immune or inflammatory responses, platelet degranulation and coagulation, and metabolism, that likely contribute to the pathogenesis. Our findings provide valuable knowledge about COVID-19 biomarkers and shed light on the pathogenesis and potential therapeutic targets of COVID-19.
Keywords: COVID-19; SARS-CoV-2; biomarkers; plasma; proteomics.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests Wuhan Institute of Virology and Wuhan Jinyintan Hospital on behalf of the authors X. Zhou., Y.S., D.-Y.Z., Y.X., Y.Q., T.S., D.W., and M.H. have filed three Chinese patent applications (202010478392.8, 202010476095.X, and 202010476805.9) related to the biomarkers for predicting the different outcomes of COVID-19 patients.
Figures







Comment in
-
Biomarkers of COVID-19 severity may not serve patients with polycystic ovary syndrome.J Transl Med. 2021 Feb 11;19(1):63. doi: 10.1186/s12967-021-02723-7. J Transl Med. 2021. PMID: 33573655 Free PMC article. No abstract available.
References
-
- Batth T.S., Francavilla C., Olsen J.V. Off-line high-pH reversed-phase fractionation for in-depth phosphoproteomics. J. Proteome Res. 2014;13:6176–6186. - PubMed
-
- Bengtsson A.A., Sturfelt G., Lood C., Rönnblom L., van Vollenhoven R.F., Axelsson B., Sparre B., Tuvesson H., Ohman M.W., Leanderson T. Pharmacokinetics, tolerability, and preliminary efficacy of paquinimod (ABR-215757), a new quinoline-3-carboxamide derivative: studies in lupus-prone mice and a multicenter, randomized, double-blind, placebo-controlled, repeat-dose, dose-ranging study in patients with systemic lupus erythematosus. Arthritis Rheum. 2012;64:1579–1588. - PubMed
-
- Calderone A., Castagnoli L., Cesareni G. mentha: a resource for browsing integrated protein-interaction networks. Nat. Methods. 2013;10:690–691. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
