

What do older adults with multimorbidity and polypharmacy think about deprescribing? The LESS study - a primary care-based survey
- PMID: 33129274
- PMCID: PMC7602330
- DOI: 10.1186/s12877-020-01843-x
What do older adults with multimorbidity and polypharmacy think about deprescribing? The LESS study - a primary care-based survey
Abstract
Background: Multimorbidity and polypharmacy are very common in older adults in primary care. Ideally, general practitioners (GPs), should regularly review medication lists to identify inappropriate medication(s) and, where appropriate, deprescribe. However, it remains challenging to deprescribe given time constraints and few recommendations from guidelines. Further, patient related barriers and enablers to deprescribing have to be accounted for. The aim of this study was to identify barriers and enablers to deprescribing as reported by older adults with polypharmacy and multimorbidity.
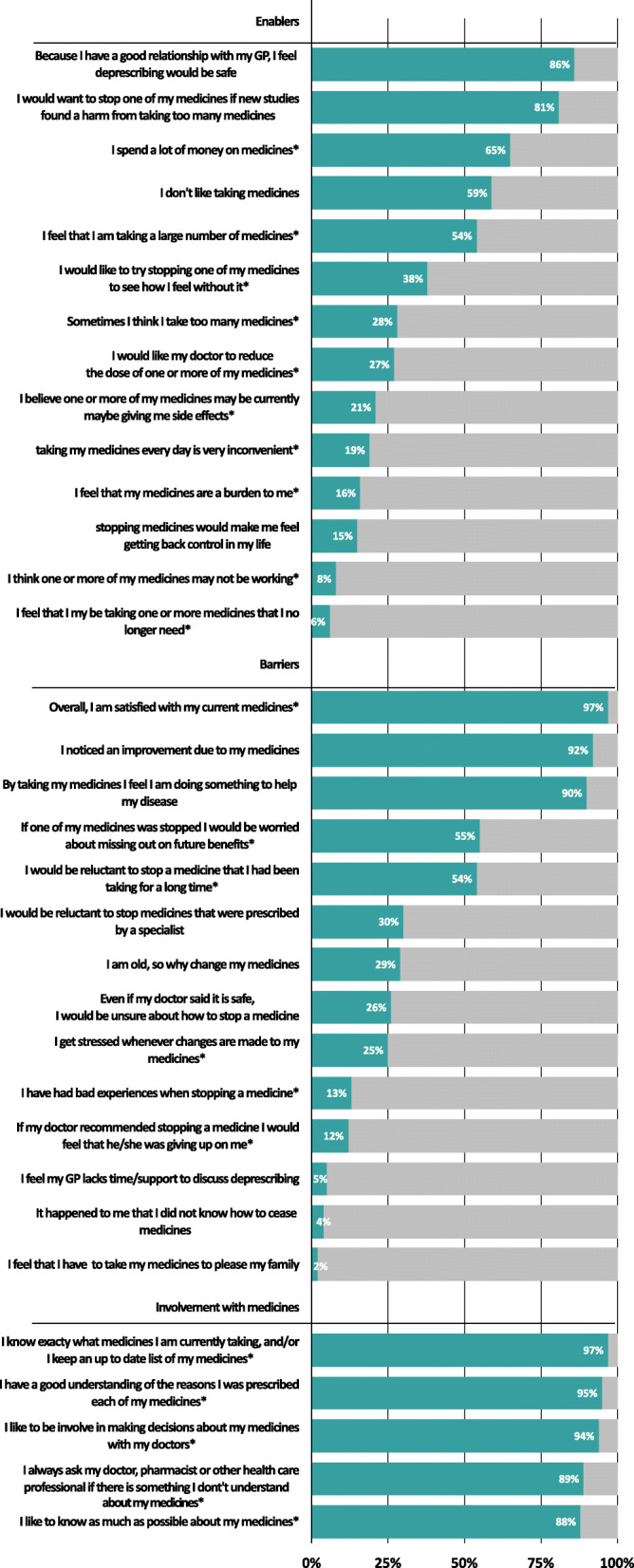
Methods: We conducted a survey among participants aged ≥70 years, with multimorbidity (≥3 chronic conditions) and polypharmacy (≥5 chronic medications). We invited Swiss GPs, to recruit eligible patients who then completed a paper-based survey on demographics, medications and chronic conditions. We used the revised Patients' Attitudes Towards Deprescribing (rPATD) questionnaire and added twelve additional Likert scale questions and two open-ended questions to assess barriers and enablers towards deprescribing, which we coded and categorized into meaningful themes.
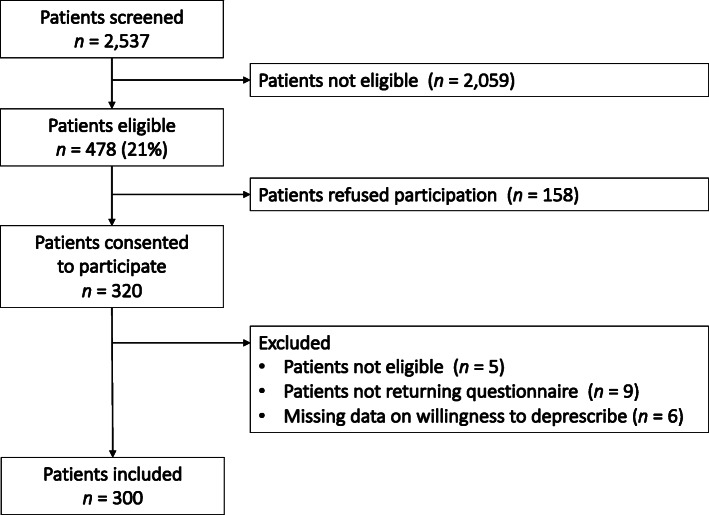
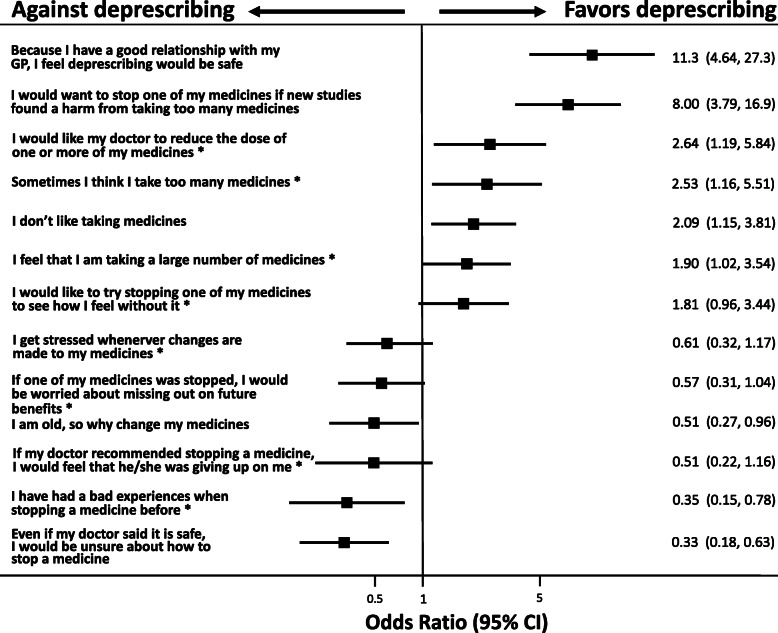
Result: Sixty four Swiss GPs consented to recruit 5-6 patients each and returned 300 participant responses. Participants were 79.1 years (SD 5.7), 47% female, 34% lived alone, and 86% managed their medications themselves. Sixty-seven percent of participants took 5-9 regular medicines and 24% took ≥10 medicines. The majority of participants (77%) were willing to deprescribe one or more of their medicines if their doctor said it was possible. There was no association with sex, age or the number of medicines and willingness to deprescribe. After adjustment for baseline characteristics, there was a strong positive association between willingness to deprescribe and saying that because they have a good relationship with their GP, they would feel that deprescribing was safe OR 11.3 (95% CI: 4.64-27.3) and agreeing that they would be willing to deprescribe if new studies showed an avoidable risk OR 8.0 (95% CI 3.79-16.9). From the open questions, the most mentioned barriers towards deprescribing were patients feeling well on their current medicines and being convinced that they need all their medicines.
Conclusions: Most older adults with polypharmacy are willing to deprescribe. GPs may be able to increase deprescribing by building trust with their patients and communicating evidence about the risks of medication use.
Keywords: Deprescribing; General practice; Multimorbidity; Older adults; Patient attitudes; Polypharmacy.
Conflict of interest statement
The authors declare to have no conflict of interest.
Figures
Similar articles
-
General practitioners' deprescribing decisions in older adults with polypharmacy: a case vignette study in 31 countries.BMC Geriatr. 2021 Jan 7;21(1):19. doi: 10.1186/s12877-020-01953-6. BMC Geriatr. 2021. PMID: 33413142 Free PMC article.
-
Influence of chronic medical conditions on older patients' willingness to deprescribe medications: a cross-sectional study.BMC Geriatr. 2024 Apr 4;24(1):315. doi: 10.1186/s12877-024-04891-9. BMC Geriatr. 2024. PMID: 38575904 Free PMC article.
-
Attitudes of ambulatory care older Nepalese patients towards deprescribing and predictors of their willingness to deprescribe.Ther Adv Drug Saf. 2021 Jun 17;12:20420986211019309. doi: 10.1177/20420986211019309. eCollection 2021. Ther Adv Drug Saf. 2021. PMID: 34211689 Free PMC article.
-
Deprescribing medicines in older people living with multimorbidity and polypharmacy: the TAILOR evidence synthesis.Health Technol Assess. 2022 Jul;26(32):1-148. doi: 10.3310/AAFO2475. Health Technol Assess. 2022. PMID: 35894932 Free PMC article. Review.
-
How Willing Are Patients or Their Caregivers to Deprescribe: a Systematic Review and Meta-analysis.J Gen Intern Med. 2021 Dec;36(12):3830-3840. doi: 10.1007/s11606-021-06965-5. Epub 2021 Jun 25. J Gen Intern Med. 2021. PMID: 34173200 Free PMC article.
Cited by
-
Cross-cultural adaptation and psychometric validation of a Spanish version of the revised Patients' Attitudes Towards Deprescribing (rPATD) questionnaire.BMJ Open. 2022 Apr 21;12(4):e050678. doi: 10.1136/bmjopen-2021-050678. BMJ Open. 2022. PMID: 35450888 Free PMC article.
-
Expert-based medication reviews to reduce polypharmacy in older patients in primary care: a northern-Italian cluster-randomised controlled trial.BMC Geriatr. 2021 Nov 23;21(1):659. doi: 10.1186/s12877-021-02612-0. BMC Geriatr. 2021. PMID: 34814835 Free PMC article. Review.
-
Baseline characteristics and comparability of older multimorbid patients with polypharmacy and general practitioners participating in a randomized controlled primary care trial.BMC Fam Pract. 2021 Jun 22;22(1):123. doi: 10.1186/s12875-021-01488-8. BMC Fam Pract. 2021. PMID: 34157981 Free PMC article. Clinical Trial.
-
Harm and Medication-Type Impact Agreement with Hypothetical Deprescribing Recommendations: a Vignette-Based Experiment with Older Adults Across Four Countries.J Gen Intern Med. 2023 May;38(6):1439-1448. doi: 10.1007/s11606-022-07850-5. Epub 2022 Nov 14. J Gen Intern Med. 2023. PMID: 36376636 Free PMC article. Clinical Trial.
-
Optimizing treatment for older adults with depression.Ther Adv Psychopharmacol. 2023 Nov 18;13:20451253231212327. doi: 10.1177/20451253231212327. eCollection 2023. Ther Adv Psychopharmacol. 2023. PMID: 38022834 Free PMC article. Review.
