

Differential effects of different delivery methods on progression to severe postpartum hemorrhage between Chinese nulliparous and multiparous women: a retrospective cohort study
- PMID: 33129300
- PMCID: PMC7603680
- DOI: 10.1186/s12884-020-03351-7
Differential effects of different delivery methods on progression to severe postpartum hemorrhage between Chinese nulliparous and multiparous women: a retrospective cohort study
Erratum in
-
Correction to: Differential effects of different delivery methods on progression to severe postpartum hemorrhage between Chinese nulliparous and multiparous women: a retrospective cohort study.BMC Pregnancy Childbirth. 2021 Jan 19;21(1):64. doi: 10.1186/s12884-021-03560-8. BMC Pregnancy Childbirth. 2021. PMID: 33468050 Free PMC article. No abstract available.
Abstract
Background: Delivery methods are associated with postpartum hemorrhage (PPH) both in nulliparous and multiparous women. However, few studies have examined the difference in this association between nulliparous and multiparous women. This study aimed to explore the difference of maternal and neonatal characteristics and delivery methods between Chinese nulliparous and multiparous women, and then examine the differential effects of different delivery methods on PPH between these two-type women.
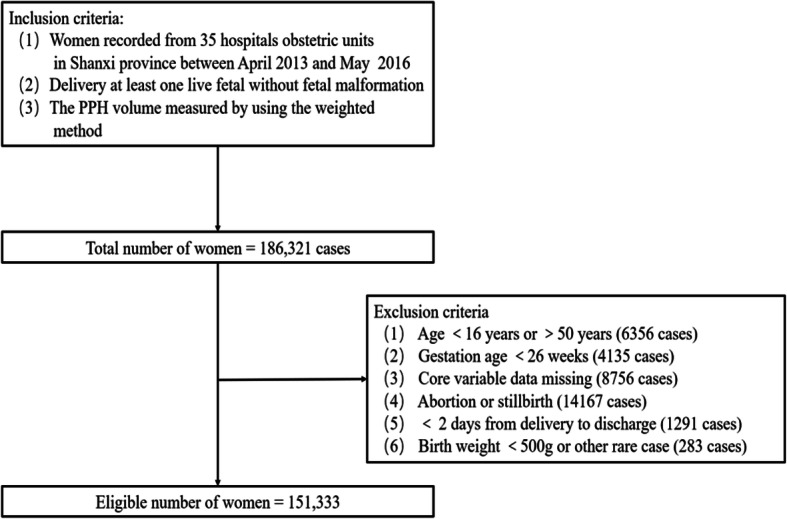
Methods: Totally 151,333 medical records of women who gave birth between April 2013 to May 2016 were obtained from the electronic health records (EHR) in a northern province, China. The severity of PPH was estimated and classified into blood loss at the level of < 900 ml, 900-1500 ml, 1500-2100 ml, and > 2100 ml. Neonatal and maternal characteristics related to PPH were derived from the same database. Multiple ordinal logistic regression was used to estimate associations.
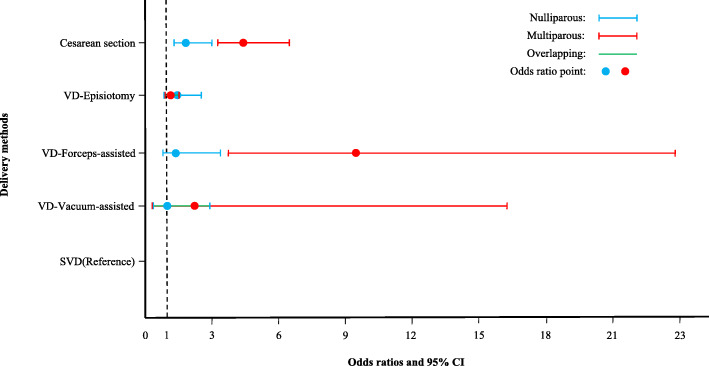
Results: Medical comorbidities, placenta previa and accreta were higher in the nulliparous group and the episiotomy rate was higher in the multiparous group. Compared with spontaneous vaginal delivery (SVD), the adjusted odds (aOR) for progression to severe PPH due to the forceps-assisted delivery was much higher in multiparous women (aOR: 9.32; 95% CI: 3.66-23.71) than in nulliparous women (aOR: 1.70; 95% CI: 0.91-3.18). The (aOR) for progression to severe PPH due to cesarean section (CS) compared to SVD was twice as high in the multiparous women (aOR: 4.32; 95% CI: 3.03-6.14) as in the nulliparous women (aOR: 2.04; 95% CI: 1.40-2.97). However, the (aOR) for progression to severe PPH due to episiotomy compared to SVD between multiparous (aOR: 1.24; 95% CI: 0.96-1.62) and nulliparous women (aOR: 1.55; 95% CI: 0.92-2.60) was not significantly different. The (aOR) for progression to severe PPH due to vacuum-assisted delivery compared to SVD in multiparous women (aOR: 2.41; 95% CI: 0.36-16.29) was not significantly different from the nulliparous women (aOR: 1.05; 95% CI: 0.40-2.73).
Conclusions: Forceps-assisted delivery and CS methods were found to increase the risk of severity of the PPH. The adverse effects were even greater for multiparous women. Episiotomy and the vacuum-assisted delivery, and SVD were similar to the risk of progression to severe PPH in either nulliparous or multiparous women. Our findings have implications for the obstetric decision on the choice of delivery methods, maternal and neonatal health care, and obstetric quality control.
Keywords: Delivery methods; Multiparous; Nulliparous; Postpartum hemorrhage.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
