

Orthogonal SARS-CoV-2 Serological Assays Enable Surveillance of Low-Prevalence Communities and Reveal Durable Humoral Immunity
- PMID: 33129373
- PMCID: PMC7554472
- DOI: 10.1016/j.immuni.2020.10.004
Orthogonal SARS-CoV-2 Serological Assays Enable Surveillance of Low-Prevalence Communities and Reveal Durable Humoral Immunity
Abstract
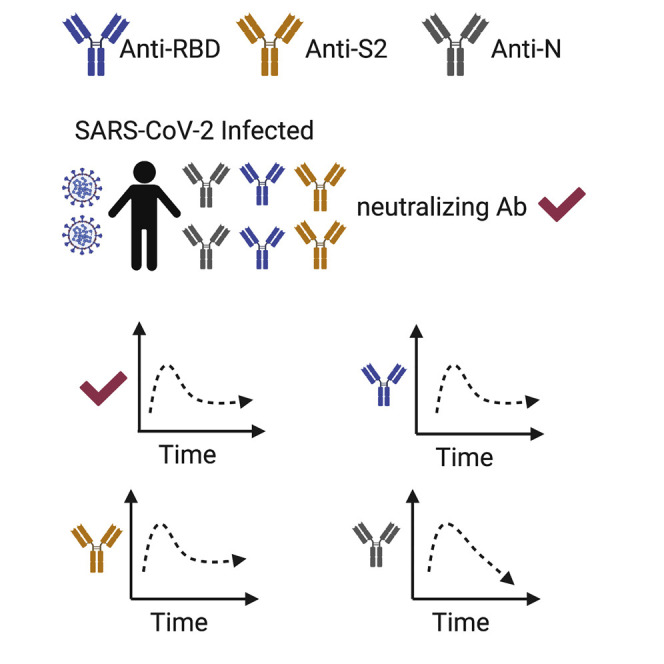
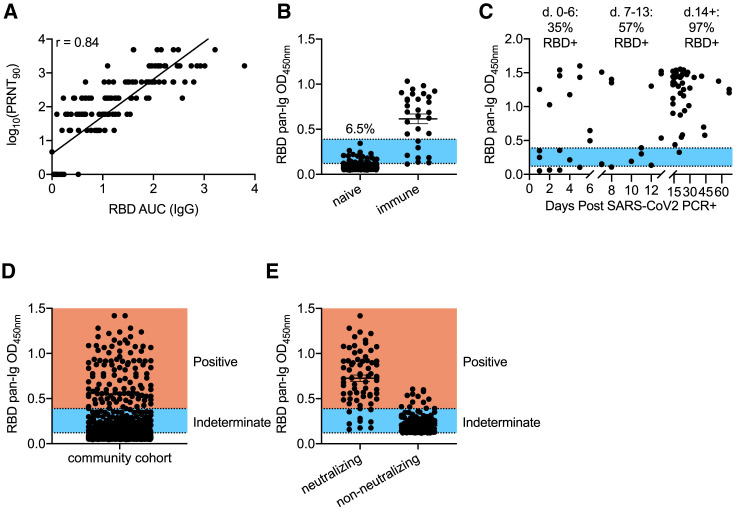
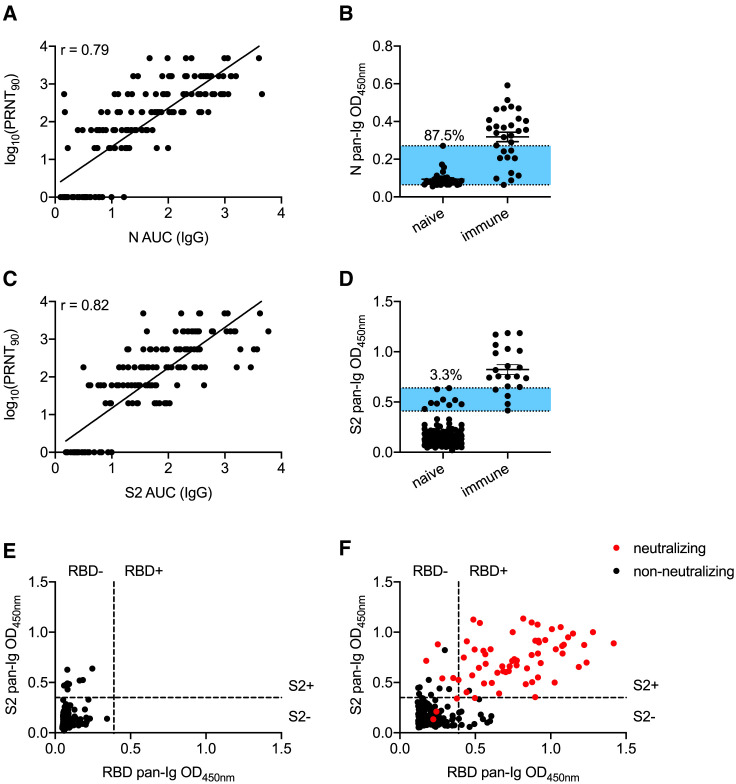
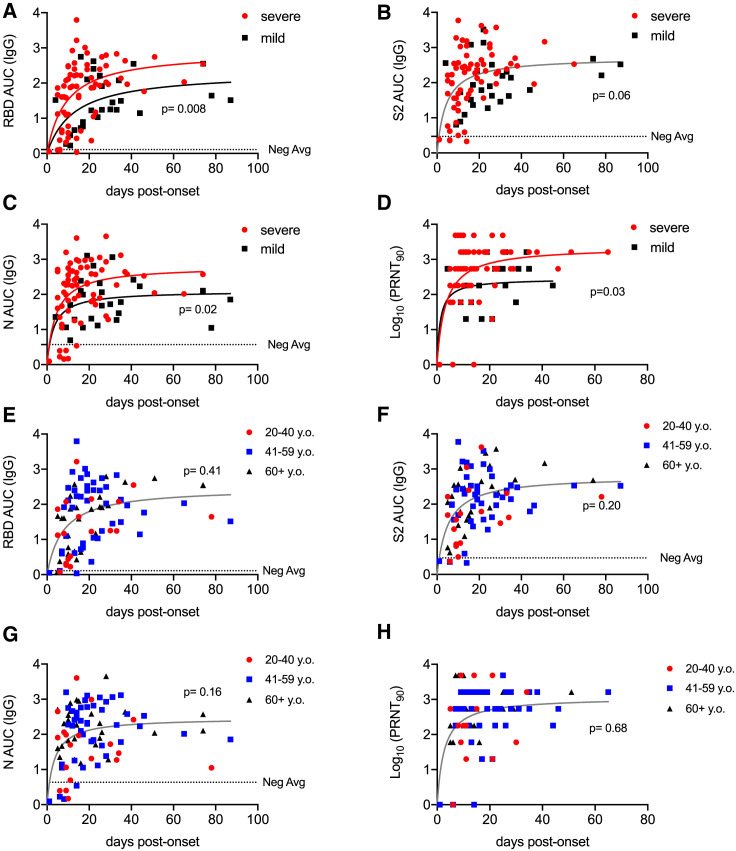
We conducted a serological study to define correlates of immunity against SARS-CoV-2. Compared to those with mild coronavirus disease 2019 (COVID-19) cases, individuals with severe disease exhibited elevated virus-neutralizing titers and antibodies against the nucleocapsid (N) and the receptor binding domain (RBD) of the spike protein. Age and sex played lesser roles. All cases, including asymptomatic individuals, seroconverted by 2 weeks after PCR confirmation. Spike RBD and S2 and neutralizing antibodies remained detectable through 5-7 months after onset, whereas α-N titers diminished. Testing 5,882 members of the local community revealed only 1 sample with seroreactivity to both RBD and S2 that lacked neutralizing antibodies. This fidelity could not be achieved with either RBD or S2 alone. Thus, inclusion of multiple independent assays improved the accuracy of antibody tests in low-seroprevalence communities and revealed differences in antibody kinetics depending on the antigen. We conclude that neutralizing antibodies are stably produced for at least 5-7 months after SARS-CoV-2 infection.
Keywords: COVID-19; S2 domain; SARS-CoV-2; antibodies; neutralization; nucleocapsid protein; orthogonal serological tests; receptor binding domain; serological test; serology; spike protein.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests Unrelated intellectual property of D.B. and Washington University has been licensed by Sana Biotechnology. J.N.Ž. is on the scientific advisory board of and receives research funding from Young Blood, Inc. R.S. is a founder and chief scientific officer of Geneticure. R.W. is currently an employee of Vir Biotechnology. A provisional patent application related to this work has been filed with the US Patent Office.
Figures

Update of
-
Detection, prevalence, and duration of humoral responses to SARS-CoV-2 under conditions of limited population exposure.medRxiv [Preprint]. 2020 Aug 15:2020.08.14.20174490. doi: 10.1101/2020.08.14.20174490. medRxiv. 2020. Update in: Immunity. 2020 Nov 17;53(5):925-933.e4. doi: 10.1016/j.immuni.2020.10.004. PMID: 32817969 Free PMC article. Updated. Preprint.
Comment in
-
Longitudinal dynamics of antibody responses in recovered COVID-19 patients.Signal Transduct Target Ther. 2021 Mar 31;6(1):137. doi: 10.1038/s41392-021-00559-7. Signal Transduct Target Ther. 2021. PMID: 33790222 Free PMC article. No abstract available.
References
-
- Abbott R.K., Lee J.H., Menis S., Skog P., Rossi M., Ota T., Kulp D.W., Bhullar D., Kalyuzhniy O., Havenar-Daughton C. Precursor Frequency and Affinity Determine B Cell Competitive Fitness in Germinal Centers, Tested with Germline-Targeting HIV Vaccine Immunogens. Immunity. 2018;48:133–146.e6. - PMC - PubMed
-
- Amanna I.J., Carlson N.E., Slifka M.K. Duration of humoral immunity to common viral and vaccine antigens. N. Engl. J. Med. 2007;357:1903–1915. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
