

Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19
- PMID: 33129663
- PMCID: PMC7598769
- DOI: 10.1016/j.jacc.2020.09.549
Prognostic Impact of Prior Heart Failure in Patients Hospitalized With COVID-19
Abstract
Background: Patients with pre-existing heart failure (HF) are likely at higher risk for adverse outcomes in coronavirus disease-2019 (COVID-19), but data on this population are sparse.
Objectives: This study described the clinical profile and associated outcomes among patients with HF hospitalized with COVID-19.
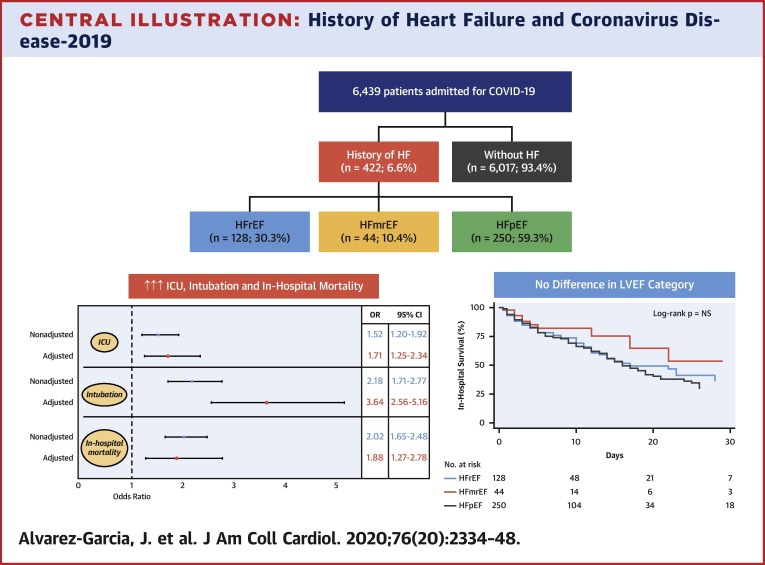
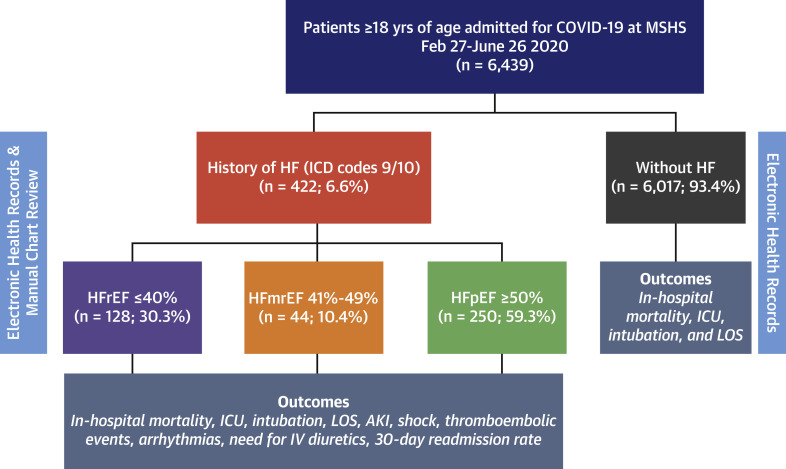
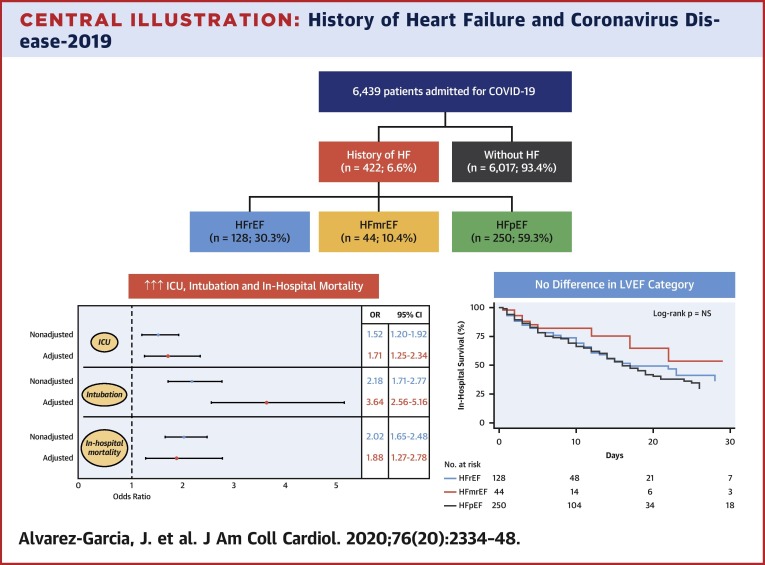
Methods: This study conducted a retrospective analysis of 6,439 patients admitted for COVID-19 at 1 of 5 Mount Sinai Health System hospitals in New York City between February 27 and June 26, 2020. Clinical characteristics and outcomes (length of stay, need for intensive care unit, mechanical ventilation, and in-hospital mortality) were captured from electronic health records. For patients identified as having a history of HF by International Classification of Diseases-9th and/or 10th Revisions codes, manual chart abstraction informed etiology, functional class, and left ventricular ejection fraction (LVEF).
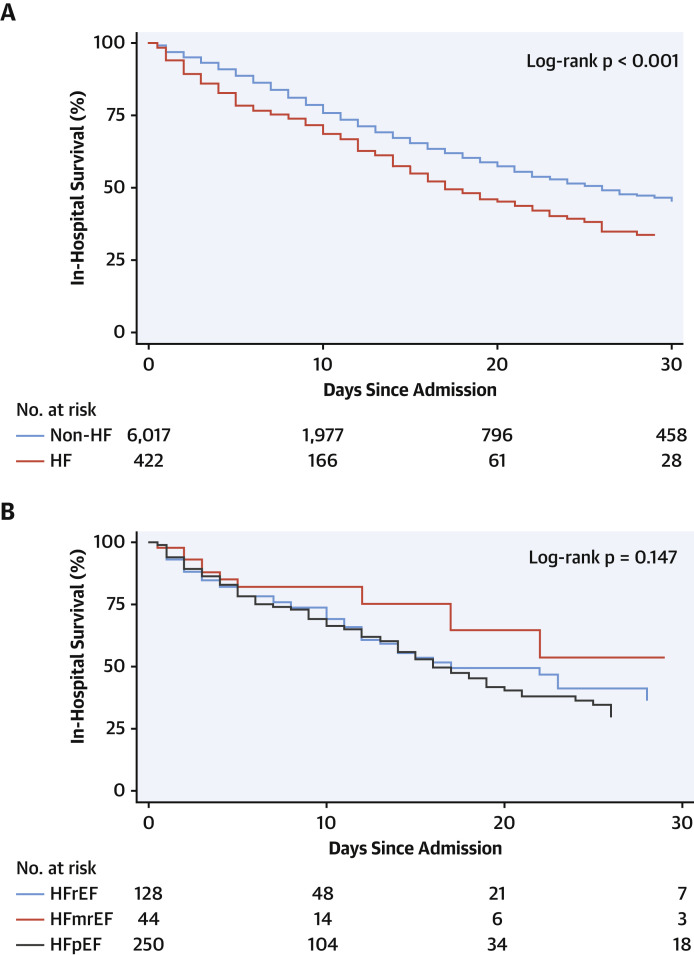
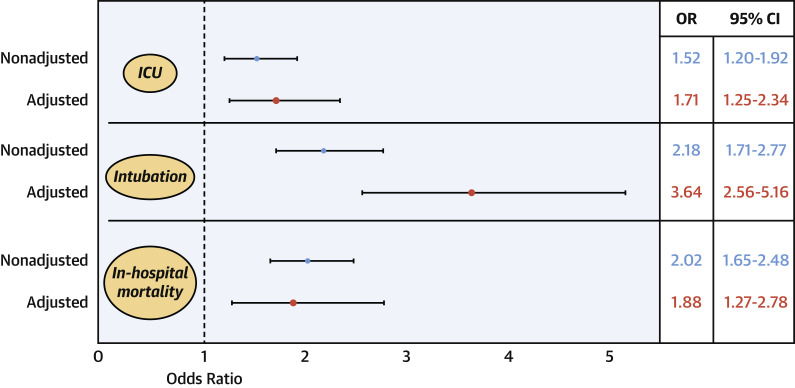
Results: Mean age was 63.5 years, and 45% were women. Compared with patients without HF, those with previous HF experienced longer length of stay (8 days vs. 6 days; p < 0.001), increased risk of mechanical ventilation (22.8% vs. 11.9%; adjusted odds ratio: 3.64; 95% confidence interval: 2.56 to 5.16; p < 0.001), and mortality (40.0% vs. 24.9%; adjusted odds ratio: 1.88; 95% confidence interval: 1.27 to 2.78; p = 0.002). Outcomes among patients with HF were similar, regardless of LVEF or renin-angiotensin-aldosterone inhibitor use.
Conclusions: History of HF was associated with higher risk of mechanical ventilation and mortality among patients hospitalized for COVID-19, regardless of LVEF.
Keywords: COVID-19; coronavirus; heart failure; left ventricular ejection fraction; outcome; renin-angiotensin-aldosterone system inhibitor.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Relationship With Industry Dr. Alvarez-Garcia received a mobility grant from Private Foundation Daniel Bravo Andreu (Spain). Dr. Rivas-Lasarte received a “Magda Heras” mobility grant from Spanish Society of Cardiology (Spain). Dr. Mitter has received personal fees from Abbott Laboratories, Cowen & Co., and the Heart Failure Society of America. Dr. Nadkarni has received grants, personal fees, and nonfinancial support from Renalytix AI; has received nonfinancial support from Pensieve Health; and has received personal fees from AstraZeneca, Variant Bio, BioVie, and GLG Consulting, outside the submitted work. Dr. Fayad has received grants from Daiichi-Sankyo, Amgen, Bristol Myers Squibb, and Siemens Healthineers; has received personal fees from Alexion, GlaxoSmithKline, and Trained Therapeutix Discovery, outside the submitted work; and holds patents licensed to Trained Therapeutix Discovery. Dr. Lala has received personal fees from Zoll, outside the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
COVID-19 and Heart Failure: Harsh Reality of Pre-Existing Conditions.J Am Coll Cardiol. 2020 Nov 17;76(20):2349-2351. doi: 10.1016/j.jacc.2020.09.588. J Am Coll Cardiol. 2020. PMID: 33183508 Free PMC article.
References
-
- John Hopkins University COVID-19 Map. Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html Available at:
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
