

Prognostic Value of Computed Tomography-Derived Extracellular Volume in TAVR Patients With Low-Flow Low-Gradient Aortic Stenosis
- PMID: 33129731
- PMCID: PMC7850162
- DOI: 10.1016/j.jcmg.2020.07.045
Prognostic Value of Computed Tomography-Derived Extracellular Volume in TAVR Patients With Low-Flow Low-Gradient Aortic Stenosis
Abstract
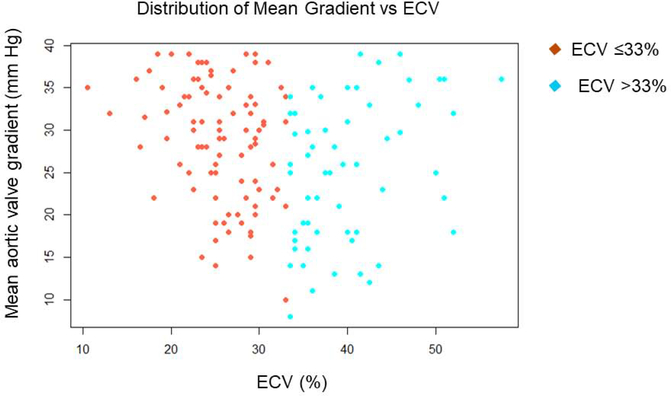
Objectives: The association between extracellular volume (ECV) measured by computed tomography angiography (CTA) and clinical outcomes was evaluated in low-flow low-gradient (LFLG) aortic stenosis (AS) patients undergoing transcatheter aortic valve replacement (TAVR).
Background: Patients with LFLG AS comprise a high-risk group with respect to clinical outcomes. Although ECV, a marker of myocardial fibrosis, is traditionally measured with cardiac magnetic resonance, it can also be measured using cardiac CTA. The authors hypothesized that in LFLG AS, increased ECV may be associated with adverse clinical outcomes.
Methods: In 150 LFLG patients with AS who underwent TAVR, ECV was quantified using pre-TAVR CTA. Echocardiographic and clinical information including all-cause death and heart failure rehospitalization (HFH) was obtained from electronic medical records. A Cox proportional hazards model was used to evaluate the association between ECV and death+HFH.
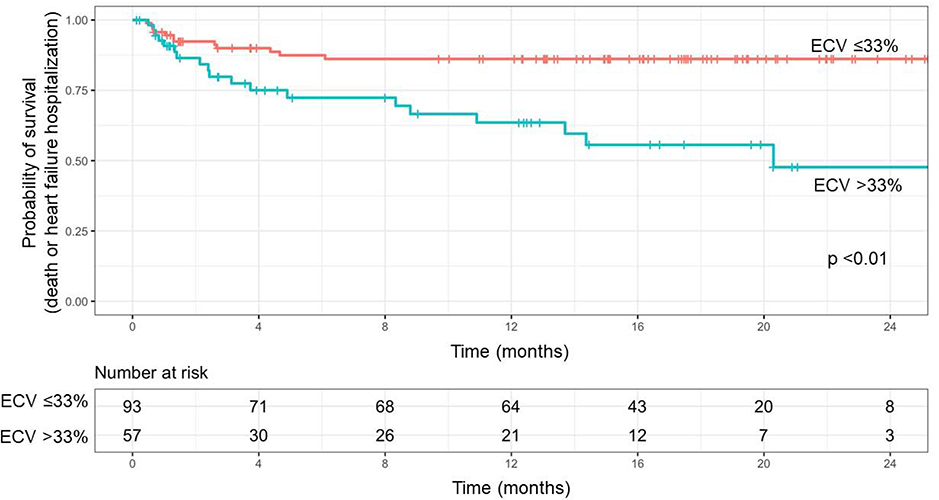
Results: During a median follow-up of 13.9 months (range 0.07 to 28.9 months), there were 31 death+HFH events (21%). Patients who experienced death+HFH had a greater median Society of Thoracic Surgery score (9.9 vs. 4.7; p < 0.01), lower left ventricular ejection fraction (42.3 ± 20.2% vs. 52.7 ± 17.2%; p < 0.01), lower mean transvalvular gradient (24.9 ± 8.9 mm Hg vs. 28.1 ± 7.3 mm Hg; p = 0.04) and increased mean ECV (35.5 ± 9.6% vs. 29.9 ± 8.2%; p < 0.01) compared with patients who did not experience death+HFH. In a multivariable Cox proportional hazards model, increase in ECV was associated with increase in death+HFH, (hazard ratio per 1% increase: 1.04, 95% confidence interval: 1.01 to 1.09; p < 0.01).
Conclusions: In patients with LFLG AS, CTA measured increase in ECV is associated with increased risk of adverse clinical outcomes post-TAVR and may thus serve as a useful noninvasive marker for prognostication.
Keywords: aortic stenosis; computed tomography; extracellular volume; low-flow low-gradient; transcatheter aortic valve replacement.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author Disclosures This work was funded by National Heart, Lung, and Blood Institute grant 7R56HL131871-02 (to Dr. Tamarappoo) and by the Miriam & Sheldon G. Adelson Medical Research Foundation (to Dr. Berman). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures



Comment in
-
Extracellular Volume Imaging in Aortic Stenosis During Routine Pre-TAVR Cardiac Computed Tomography.JACC Cardiovasc Imaging. 2020 Dec;13(12):2602-2604. doi: 10.1016/j.jcmg.2020.08.023. Epub 2020 Oct 28. JACC Cardiovasc Imaging. 2020. PMID: 33129733 No abstract available.
References
-
- Pibarot P, Dumesnil JG. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J Am Coll Cardiol 2012;60:1845–53. - PubMed
-
- Dayan V, Vignolo G, Magne J, Clavel MA, Mohty D, Pibarot P. Outcome and Impact of Aortic Valve Replacement in Patients With Preserved LVEF and Low-Gradient Aortic Stenosis. J Am Coll Cardiol 2015;66:2594–2603. - PubMed
-
- Herrmann HC, Pibarot P, Hueter I et al. Predictors of mortality and outcomes of therapy in low-flow severe aortic stenosis: a Placement of Aortic Transcatheter Valves (PARTNER) trial analysis. Circulation 2013;127:2316–26. - PubMed
-
- O’Sullivan CJ, Stortecky S, Heg D et al. Clinical outcomes of patients with low-flow, low-gradient, severe aortic stenosis and either preserved or reduced ejection fraction undergoing transcatheter aortic valve implantation. Eur Heart J 2013;34:3437–50. - PubMed
-
- Clavel MA, Berthelot-Richer M, Le Ven F et al. Impact of classic and paradoxical low flow on survival after aortic valve replacement for severe aortic stenosis. J Am Coll Cardiol 2015;65:645–53. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
