

Characteristics of Cardiac Injury in Critically Ill Patients With Coronavirus Disease 2019
- PMID: 33129792
- PMCID: PMC7591864
- DOI: 10.1016/j.chest.2020.10.056
Characteristics of Cardiac Injury in Critically Ill Patients With Coronavirus Disease 2019
Abstract
Background: Cardiac injury has been reported in up to 30% of coronavirus disease 2019 (COVID-19) patients. However, cardiac injury is defined mainly by troponin elevation without description of associated structural abnormalities and its time course has not been studied.
Research question: What are the ECG and echocardiographic abnormalities as well as their time course in critically ill COVID-19 patients?
Study design and methods: The cardiac function of 43 consecutive COVID-19 patients admitted to two ICUs was assessed prospectively and repeatedly, combining ECG, cardiac biomarker, and transthoracic echocardiographic analyses from ICU admission to ICU discharge or death or to a maximum follow-up of 14 days. Cardiac injury was defined by troponin elevation and newly diagnosed ECG or echocardiographic abnormalities, or both.
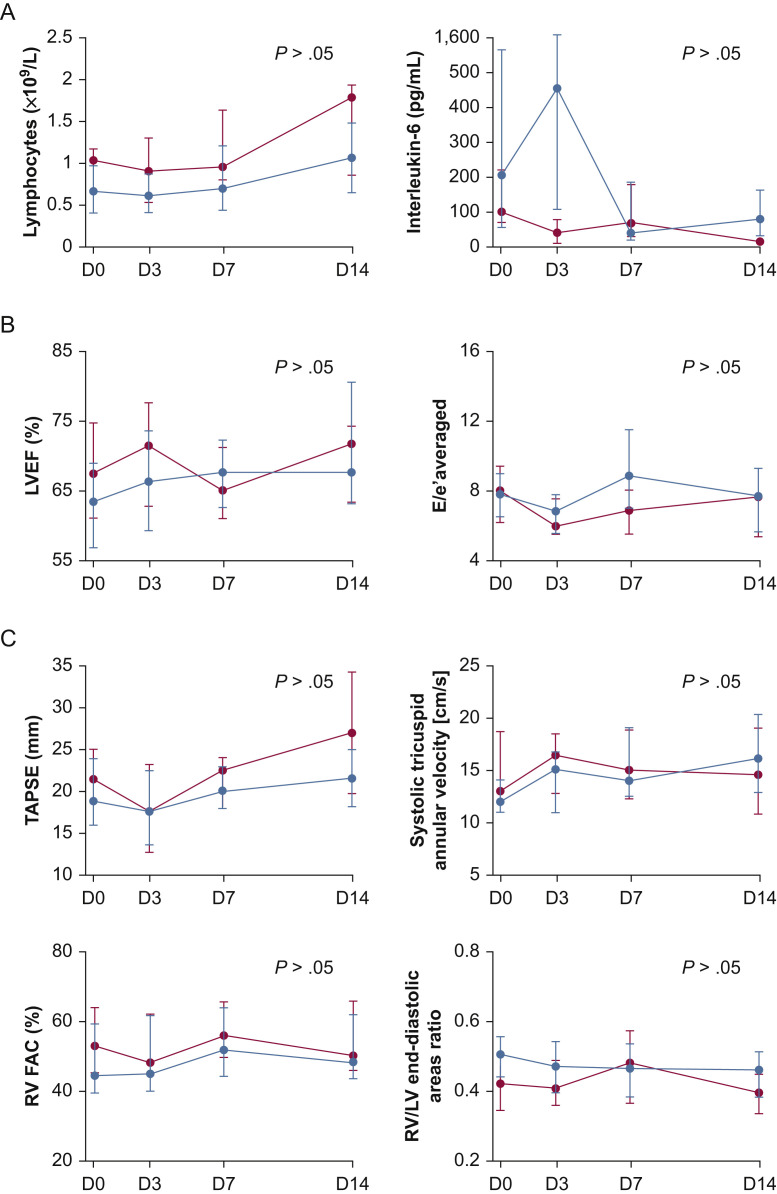
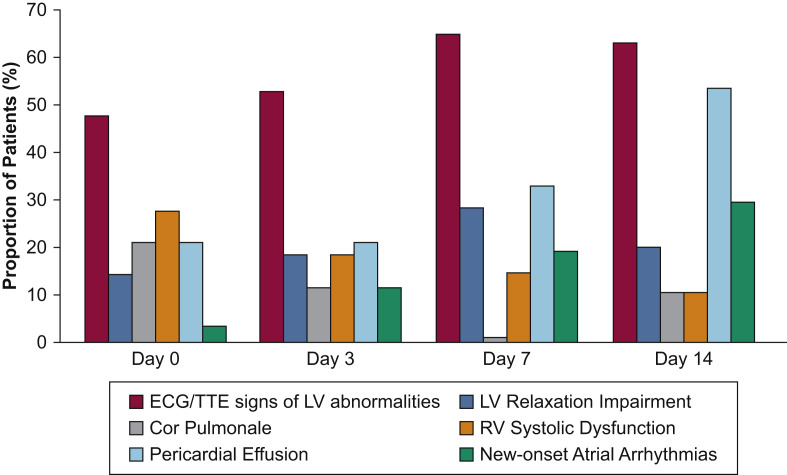
Results: At baseline, 49% of patients demonstrated a cardiac injury, and 70% of patients experienced cardiac injury within the first 14 days of ICU stay, with a median time of occurrence of 3 days (range, 0-7 days). The most frequent abnormalities were ECG or echocardiographic signs, or both, of left ventricular (LV) abnormalities (87% of patients with cardiac injury), right ventricular (RV) systolic dysfunction (47%), pericardial effusion (43%), new-onset atrial arrhythmias (33%), LV relaxation impairment (33%), and LV systolic dysfunction (13%). Between baseline and day 14, the incidence of pericardial effusion and of new-onset atrial arrhythmias increased and the incidence of ECG or echocardiographic signs, or both, of LV abnormalities as well as the incidence of LV relaxation impairment remained stable, whereas the incidence of RV and LV systolic dysfunction decreased.
Interpretation: Cardiac injury is common and early in critically ill COVID-19 patients. ECG or echocardiographic signs, or both, of LV abnormalities were the most frequent abnormalities, and patients with cardiac injury experienced more RV than LV systolic dysfunction.
Keywords: COVID-19; ECG; ICU; cardiac injury; echocardiography.
Copyright © 2020 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
What We Might Find If We Only Looked.Chest. 2021 May;159(5):1715-1716. doi: 10.1016/j.chest.2021.01.013. Chest. 2021. PMID: 33965128 Free PMC article. No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
