

Comprehensive evaluation of electrophysiological and 3D structural features of human atrial myocardium with insights on atrial fibrillation maintenance mechanisms
- PMID: 33130148
- PMCID: PMC7880876
- DOI: 10.1016/j.yjmcc.2020.10.012
Comprehensive evaluation of electrophysiological and 3D structural features of human atrial myocardium with insights on atrial fibrillation maintenance mechanisms
Abstract
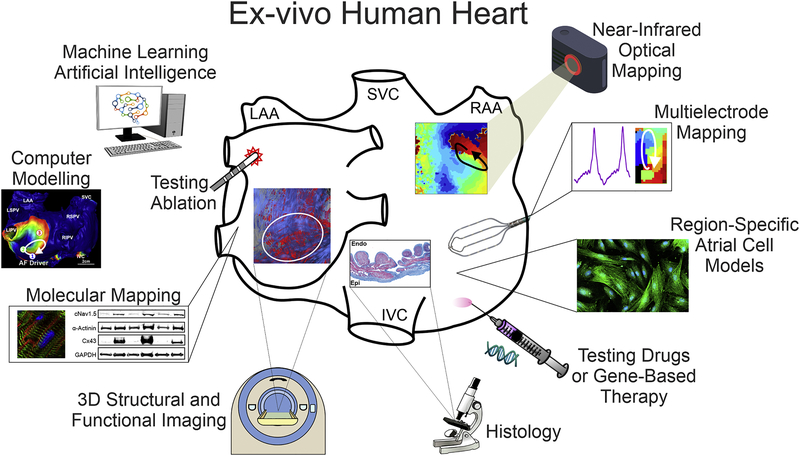
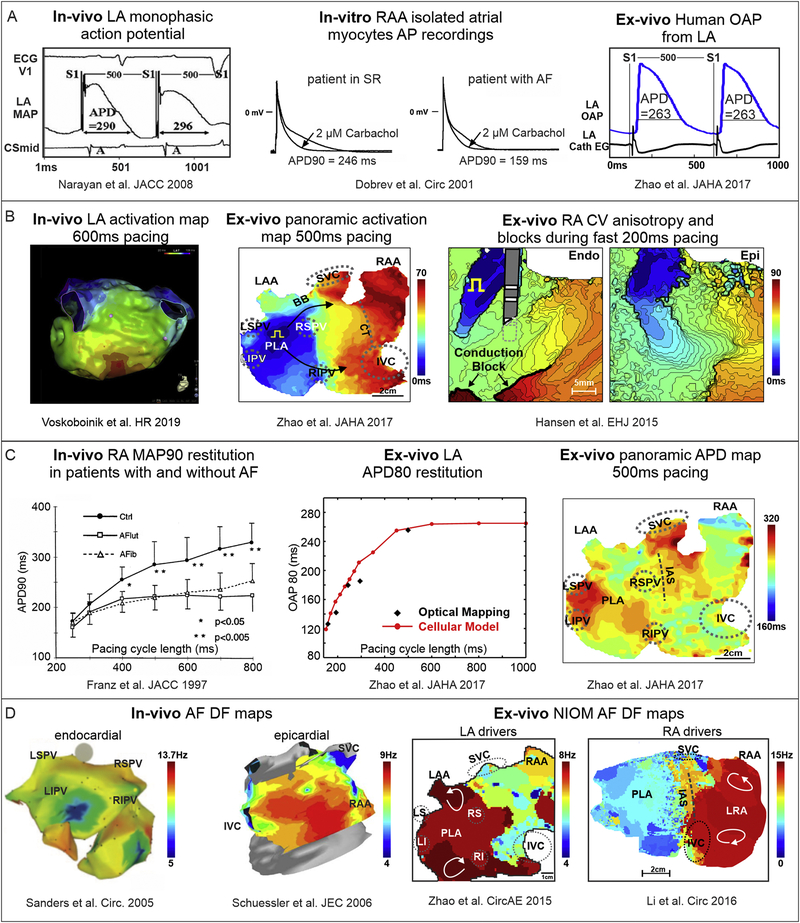
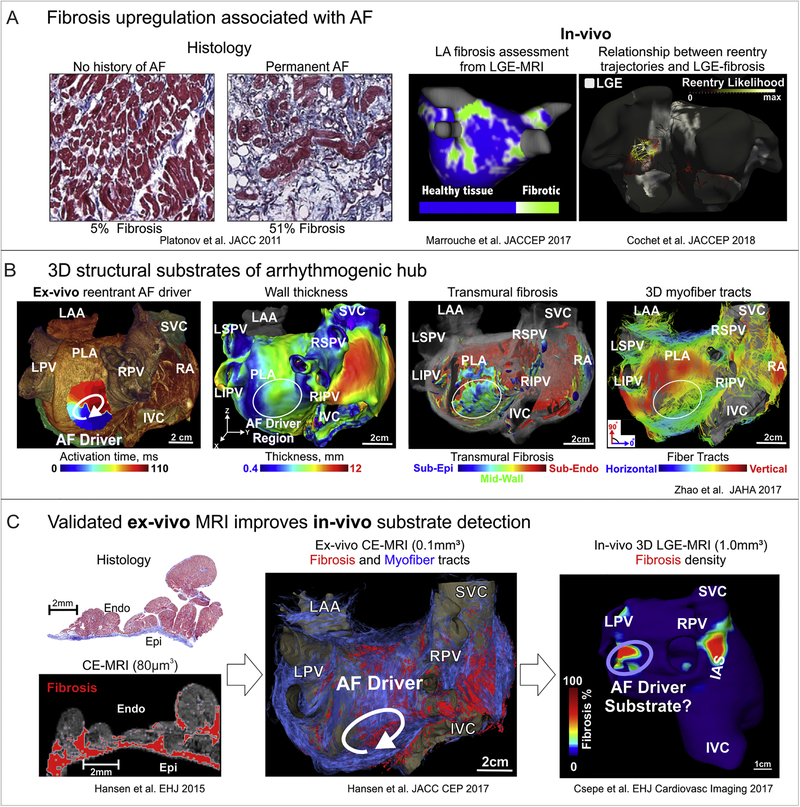
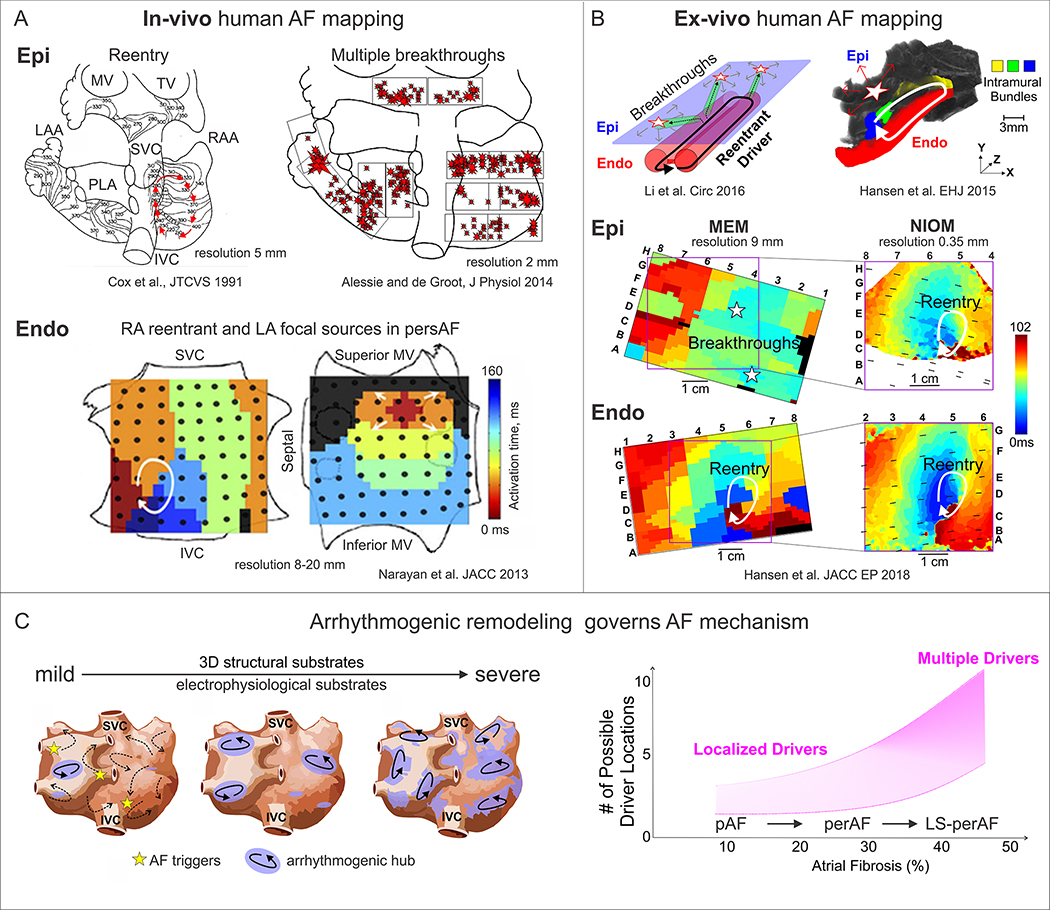
Atrial fibrillation (AF) occurrence and maintenance is associated with progressive remodeling of electrophysiological (repolarization and conduction) and 3D structural (fibrosis, fiber orientations, and wall thickness) features of the human atria. Significant diversity in AF etiology leads to heterogeneous arrhythmogenic electrophysiological and structural substrates within the 3D structure of the human atria. Since current clinical methods have yet to fully resolve the patient-specific arrhythmogenic substrates, mechanism-based AF treatments remain underdeveloped. Here, we review current knowledge from in-vivo, ex-vivo, and in-vitro human heart studies, and discuss how these studies may provide new insights on the synergy of atrial electrophysiological and 3D structural features in AF maintenance. In-vitro studies on surgically acquired human atrial samples provide a great opportunity to study a wide spectrum of AF pathology, including functional changes in single-cell action potentials, ion channels, and gene/protein expression. However, limited size of the samples prevents evaluation of heterogeneous AF substrates and reentrant mechanisms. In contrast, coronary-perfused ex-vivo human hearts can be studied with state-of-the-art functional and structural technologies, such as high-resolution near-infrared optical mapping and contrast-enhanced MRI. These imaging modalities can resolve atrial arrhythmogenic substrates and their role in reentrant mechanisms maintaining AF and validate clinical approaches. Nonetheless, longitudinal studies are not feasible in explanted human hearts. As no approach is perfect, we suggest that combining the strengths of direct human atrial studies with high fidelity approaches available in the laboratory and in realistic patient-specific computer models would elucidate deeper knowledge of AF mechanisms. We propose that a comprehensive translational pipeline from ex-vivo human heart studies to longitudinal clinically relevant AF animal studies and finally to clinical trials is necessary to identify patient-specific arrhythmogenic substrates and develop novel AF treatments.
Keywords: Atrial fibrillation; Electrophysiology; Ex-vivo human heart; Fibrosis; Near-infrared optical mapping.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
References
-
- Nishida K, Nattel S, Atrial fibrillation compendium: historical context and detailed translational perspective on an important clinical problem, Circ. Res 114(9) (2014) 1447–1452. - PubMed
-
- Pedersen OD, Abildstrom SZ, Ottesen MM, Rask-Madsen C, Bagger H, Kober L, et al. , Increased risk of sudden and non-sudden cardiovascular death in patients with atrial fibrillation/flutter following acute myocardial infarction, Eur Heart J 27(3) (2006) 290–5. - PubMed
-
- Ling LH, Kistler PM, Kalman JM, Schilling RJ, Hunter RJ, Comorbidity of atrial fibrillation and heart failure, Nat Rev Cardiol 13(3) (2016) 131–47. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
