

Host-pathogen interaction in COVID-19: Pathogenesis, potential therapeutics and vaccination strategies
- PMID: 33130519
- PMCID: PMC7434692
- DOI: 10.1016/j.imbio.2020.152008
Host-pathogen interaction in COVID-19: Pathogenesis, potential therapeutics and vaccination strategies
Abstract
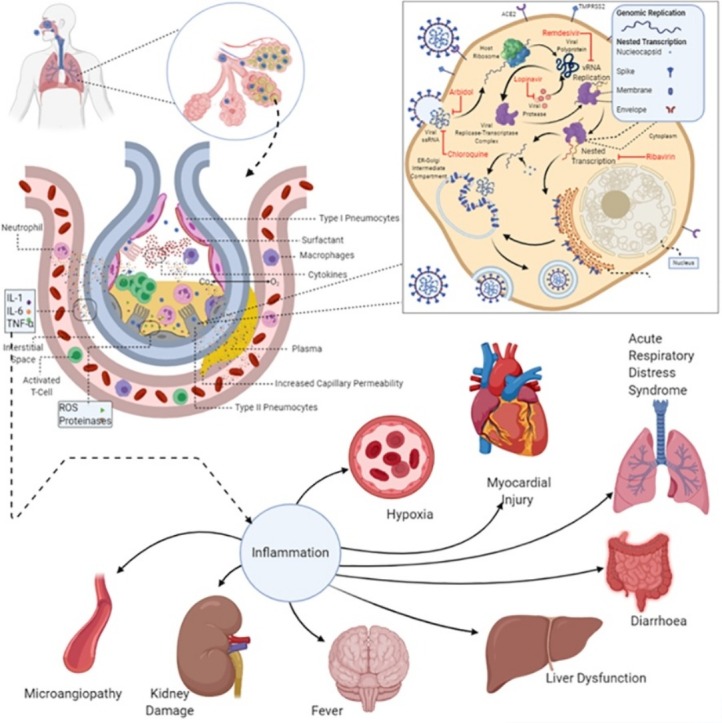
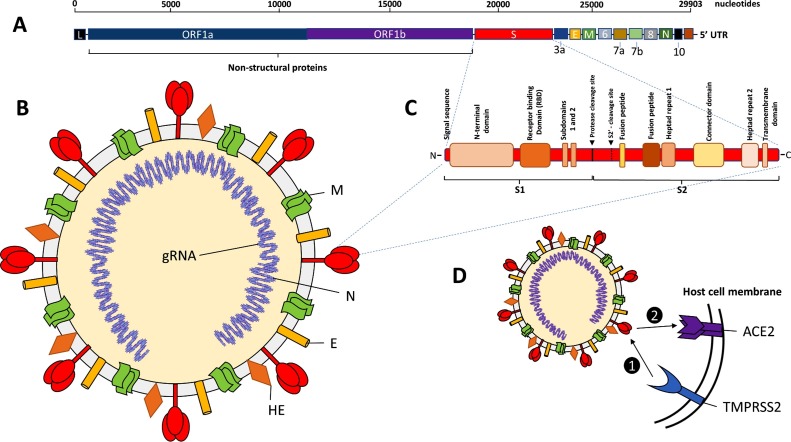
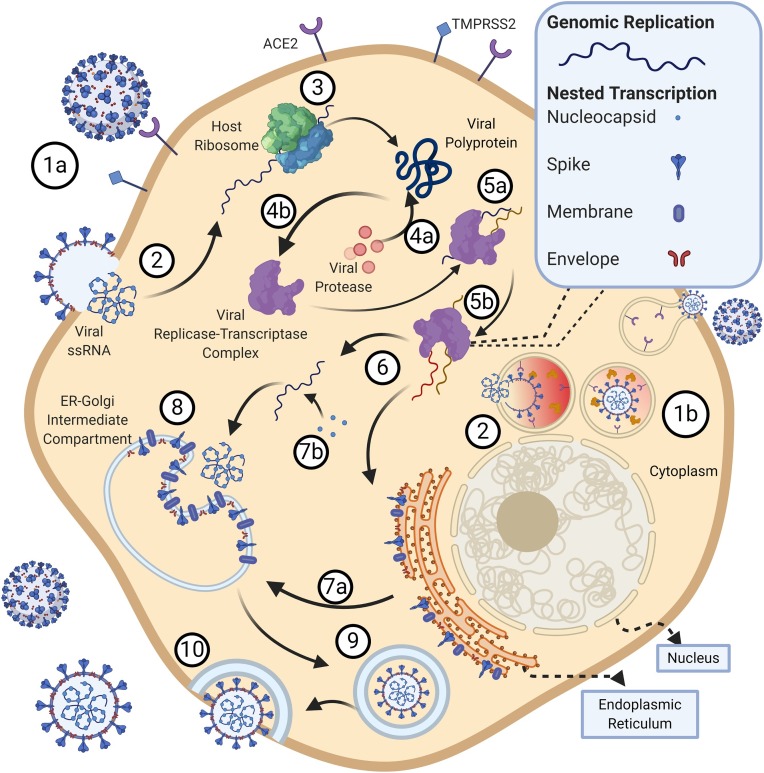
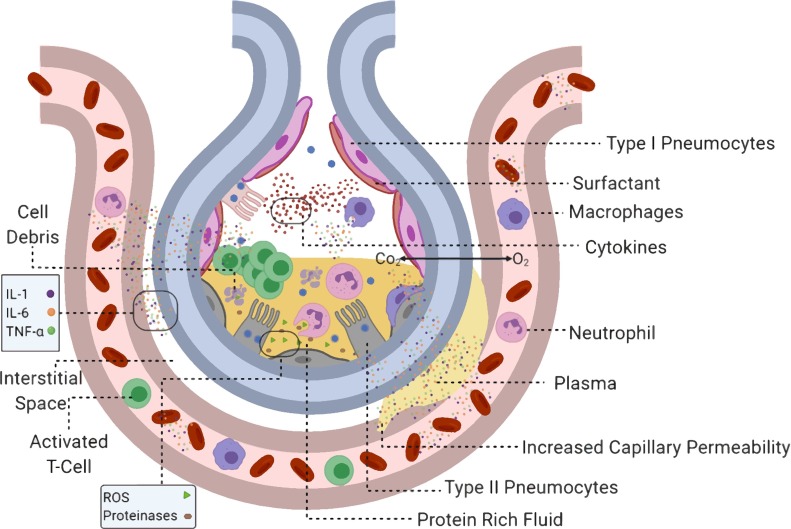
The current coronavirus pandemic, COVID-19, is the third outbreak of disease caused by the coronavirus family, after Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome. It is an acute infectious disease caused by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). This severe disease is characterised by acute respiratory distress syndrome, septic shock, metabolic acidosis, coagulation dysfunction, and multiple organ dysfunction syndromes. Currently, no drugs or vaccines exist against the disease and the only course of treatment is symptom management involving mechanical ventilation, immune suppressants, and repurposed drugs. The severe form of the disease has a relatively high mortality rate. The last six months have seen an explosion of information related to the host receptors, virus transmission, virus structure-function relationships, pathophysiology, co-morbidities, immune response, treatment and the most promising vaccines. This review takes a critically comprehensive look at various aspects of the host-pathogen interaction in COVID-19. We examine the genomic aspects of SARS-CoV-2, modulation of innate and adaptive immunity, complement-triggered microangiopathy, and host transmission modalities. We also examine its pathophysiological impact during pregnancy, in addition to emphasizing various gaps in our knowledge. The lessons learnt from various clinical trials involving repurposed drugs have been summarised. We also highlight the rationale and likely success of the most promising vaccine candidates.
Keywords: Anti-virals; COVID-19; Co-morbidities; Life-cycle; Pathophysiology; Pregnancy; SARS-CoV-2; Vaccine.
Copyright © 2020 Elsevier GmbH. All rights reserved.
Conflict of interest statement
The authors report no declarations of interest.
Figures

References
-
- Arabi Y.M., Hajeer A.H., Luke T., Raviprakash K., Balkhy H., Johani S., Al-Dawood A., Al-Qahtani S., Al-Omari A., Al-Hameed F., et al. Feasibility of using convalescent plasma immunotherapy for MERS-CoV infection, Saudi Arabia. Emerg Infect Dis. 2016 doi: 10.3201/eid2209.151164. - DOI - PMC - PubMed
-
- Assistance publique – Hôpitaux de Paris . 2020. Le Tocilizumab Améliore Significativement Le Pronostic Des Patients Avec Pneumonie COVID Moyenne Ou Sévère | APHP.https://www.aphp.fr/contenu/le-tocilizumab-ameliore-significativement-le... Available at: [Accessed May 15, 2020]
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
