

Elective staged proctocolectomy and living donor liver transplantation for colon cancer with sclerosing cholangitis-related ulcerative colitis: a case report
- PMID: 33130979
- PMCID: PMC7604274
- DOI: 10.1186/s40792-020-01059-6
Elective staged proctocolectomy and living donor liver transplantation for colon cancer with sclerosing cholangitis-related ulcerative colitis: a case report
Abstract
Background: Primary sclerosing cholangitis (PSC) is a well-known complication of ulcerative colitis (UC), but it is rare to encounter patients requiring both living donor liver transplantation (LDLT) and proctocolectomy. We report a case of elective two-stage surgery involving proctocolectomy performed after LDLT for a patient with early colon cancer concurrent with PSC-related UC. To our knowledge, this is the first report of concurrent cancer successfully treated with both LDLT and proctocolectomy.
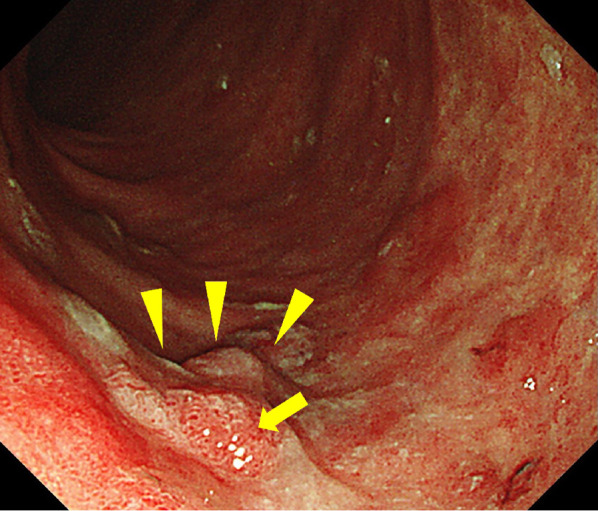
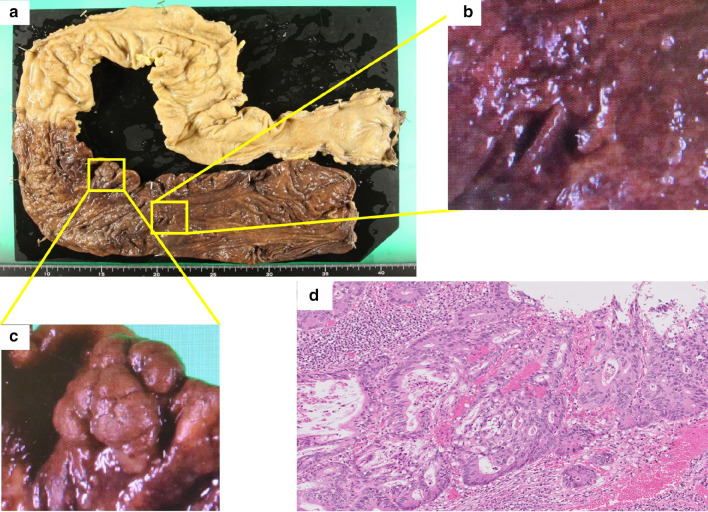
Case presentation: A 32-year-old Japanese man with colon cancer associated with UC underwent restorative proctocolectomy at 3 months after living donor liver transplantation (LDLT) for PSC. He was diagnosed with PSC and UC when he was a teenager. Conservative therapy was initiated to treat both PSC and UC. He had experienced recurrent cholangitis for years; therefore, a biliary stent was placed endoscopically. However, his liver function progressively deteriorated. Colonoscopic surveillance revealed early colon cancer; hence, surgical treatment was considered. PSC progressed to cirrhosis and portal hypertension; hence, LDLT was performed before restorative proctocolectomy. Three months after LDLT, we performed restorative proctocolectomy with ileal pouch-anal anastomosis. The postoperative course was uneventful. The patient was well, with good liver and bowel functions and without tumor recurrence, more than 1 year after proctocolectomy.
Conclusions: With strict patient selection and careful patient management and follow-up, elective proctocolectomy may be performed safely and effectively after LDLT for concurrent early colon cancer with PSC-related UC. There are no previous reports of the use of both LDLT and proctocolectomy for the successful treatment of PSC-related UC and concurrent cancer.
Keywords: Colitis-related colon cancer; Ileal pouch–anal anastomosis; Inflammatory bowel disease; Small-for-size syndrome.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Kumagai J, Taida T, Ogasawara S, Nakagawa T, Iino Y, Shingyoji A, Ishikawa K, Akizue N, Yamato M, Takahashi K, Ohta Y, Hamanaka S, Okimoto K, Nakamura M, Ohyama H, Saito K, Kusakabe Y, Maruoka D, Yasui S, Matsumura T, Sugiyama H, Sakai Y, Mikata R, Arai M, Katsuno T, Tsuyuguchi T, Kato N. Clinical characteristics and outcomes of primary sclerosing cholangitis and ulcerative colitis in Japanese patients. PLoS ONE. 2018;13:e0209352. doi: 10.1371/journal.pone.0209352. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
